You might also like
- Antidepressant ChartDocument7 pagesAntidepressant Chartinher1tance100% (4)
- Theory and Practice of Addiction Counseling I1686Document16 pagesTheory and Practice of Addiction Counseling I1686pollomaximus 444No ratings yet
- Neem TreeDocument4 pagesNeem Treedorzky22No ratings yet
- Budwig Cancer GuideDocument125 pagesBudwig Cancer GuideDavid Gristan100% (1)
- Antibiotic Prophylaxis in DentistryDocument9 pagesAntibiotic Prophylaxis in DentistryLiana OpriţăNo ratings yet
- Australian Dental Journal: Rhinosinusitis in Oral Medicine and DentistryDocument7 pagesAustralian Dental Journal: Rhinosinusitis in Oral Medicine and DentistryVishakha SabooNo ratings yet
- Oral Histology MCQsDocument27 pagesOral Histology MCQssarah100% (2)
- Motor Relearning ProgramDocument10 pagesMotor Relearning ProgramjalykAmazing75% (4)
- Aapd Guidelines - Restorative DentistryDocument8 pagesAapd Guidelines - Restorative DentistrymahmoudNo ratings yet
- Peter Pan SyndromeDocument4 pagesPeter Pan SyndromeDaltry Gárate100% (2)
- ResumeDocument3 pagesResumeAstig Kuging63% (8)
- MCQs On Oral Histology - Dental Pulp - 1-5Document5 pagesMCQs On Oral Histology - Dental Pulp - 1-5Karizma TravelNo ratings yet
- Future PharmaDocument40 pagesFuture Pharmaet43864No ratings yet
- Management of Maxillofacial TraumaDocument33 pagesManagement of Maxillofacial TraumaAdilah Afifah67% (6)
- Sample Questions MJDF Part 1 Sample Questions MJDF Part 1Document21 pagesSample Questions MJDF Part 1 Sample Questions MJDF Part 1HarkanNo ratings yet
- Periodontal Therapy StatementDocument7 pagesPeriodontal Therapy StatementDiana AlexandraNo ratings yet
- Relining in RPD!Document33 pagesRelining in RPD!sarah50% (2)
- Management of Complications in Oral and Maxillofacial SurgeryFrom EverandManagement of Complications in Oral and Maxillofacial SurgeryRating: 2 out of 5 stars2/5 (2)
- Benign Non Odontogenic Tumors: Ossifying FibromaDocument10 pagesBenign Non Odontogenic Tumors: Ossifying FibromaIsabelle TanNo ratings yet
- CHAPTER 13. Interdisciplinary ConsiderationsDocument13 pagesCHAPTER 13. Interdisciplinary ConsiderationsAlina AnechiteiNo ratings yet
- MDS Oral Medicine Question Papers 2002Document5 pagesMDS Oral Medicine Question Papers 2002Niyas UmmerNo ratings yet
- Zygomatic Arch and Orbital FracturesDocument6 pagesZygomatic Arch and Orbital FractureszacrouchyNo ratings yet
- Overseas Registration Examination Reading ListDocument3 pagesOverseas Registration Examination Reading ListyoNo ratings yet
- Thyroid CancerDocument38 pagesThyroid CancersarahNo ratings yet
- Thyroid CancerDocument38 pagesThyroid CancersarahNo ratings yet
- Thyroid CancerDocument38 pagesThyroid CancersarahNo ratings yet
- Pulp Therapy of Non-Vital Teeth (Pulpectomy)Document27 pagesPulp Therapy of Non-Vital Teeth (Pulpectomy)Mahmoud A. ZoghborNo ratings yet
- Periodontal PocketDocument31 pagesPeriodontal Pocketperiodontics07No ratings yet
- Mandibular Major ConnectorsDocument30 pagesMandibular Major ConnectorsKrishnanunni KmNo ratings yet
- MJDF Part 1 QuestionsDocument21 pagesMJDF Part 1 QuestionsHabeeb AL-AbsiNo ratings yet
- AnatomyDocument91 pagesAnatomysarahNo ratings yet
- CH 30Document22 pagesCH 30Alejandra Oliveros VargasNo ratings yet
- Gingival Crevicular FluidDocument48 pagesGingival Crevicular FluidDUKUZIMANA CONCORDENo ratings yet
- Periodontal Problems in KidsDocument49 pagesPeriodontal Problems in KidsRaksmey PhanNo ratings yet
- Physiology MCQDocument3 pagesPhysiology MCQDr Md Abedur Rahman90% (10)
- Physiology MCQDocument3 pagesPhysiology MCQDr Md Abedur Rahman90% (10)
- HAAD Exam QsDocument2 pagesHAAD Exam Qsdrkhalilezekiel93% (15)
- Abnormalities of Teeth1.2020Document5 pagesAbnormalities of Teeth1.2020Farhaana ShaboodienNo ratings yet
- Conservative Esthetic Procedures: Part 2Document9 pagesConservative Esthetic Procedures: Part 2Dt omarNo ratings yet
- Local and Systemic Chemotherapeutic Agents in Periodontics: Part - I Chemical Plaque ControlDocument101 pagesLocal and Systemic Chemotherapeutic Agents in Periodontics: Part - I Chemical Plaque ControlSuresh Bindhumadhav100% (1)
- Oral Wound Healing: Cell Biology and Clinical ManagementFrom EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaNo ratings yet
- CHAP 10 Dental Calculus SelfDocument38 pagesCHAP 10 Dental Calculus SelfarshmeentariqNo ratings yet
- Oral Mucous MembraneDocument200 pagesOral Mucous MembraneKush Pathak100% (3)
- ABGD Reference ListDocument4 pagesABGD Reference ListFiras Abu SamraNo ratings yet
- Immunology Dental Caries-2015Document24 pagesImmunology Dental Caries-2015Bagus Rahmawan50% (2)
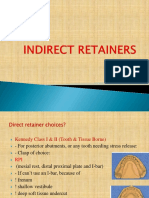
- Indirect RetainersDocument52 pagesIndirect RetainerssarahNo ratings yet
- Indirect RetainersDocument52 pagesIndirect RetainerssarahNo ratings yet
- Book Review: MCQS, Saqs, Emqs and Osces For Oral Pathology and Oral Medicine: An Exam-Focused ApproachDocument1 pageBook Review: MCQS, Saqs, Emqs and Osces For Oral Pathology and Oral Medicine: An Exam-Focused Approachshehla khanNo ratings yet
- Shalu Bathla - Chronic PeriodontitisDocument6 pagesShalu Bathla - Chronic PeriodontitisFerdinan PasaribuNo ratings yet
- Failures in Periodontal Therapy: Review ArticleDocument6 pagesFailures in Periodontal Therapy: Review ArticlezinniaNo ratings yet
- Changing Concepts in Cariology - Forty Years OnDocument7 pagesChanging Concepts in Cariology - Forty Years OnDavid CaminoNo ratings yet
- Dentalplaque Part1 161112155549Document54 pagesDentalplaque Part1 161112155549Alankrita Singh100% (1)
- Syllabus 5k en ExamDocument2 pagesSyllabus 5k en ExamVagelis RaftopoulosNo ratings yet
- Lecture 4 Diagnosis of Dental CariesDocument12 pagesLecture 4 Diagnosis of Dental CariesDt omarNo ratings yet
- Dental AuxiliariesDocument14 pagesDental AuxiliariesnainaNo ratings yet
- Dry Mouth (Xerostomia)Document18 pagesDry Mouth (Xerostomia)dr_jamal1983No ratings yet
- Medical Emergencies in Dental Practice: 1. The Drug Box, Equipment and General ApproachDocument6 pagesMedical Emergencies in Dental Practice: 1. The Drug Box, Equipment and General ApproachRodelix San Juan Dacanay100% (1)
- Apical Surgery PDFDocument7 pagesApical Surgery PDFsalman azizNo ratings yet
- Etiology of Periodontal Diseases - II - Role of Calculus and Local FactorsDocument33 pagesEtiology of Periodontal Diseases - II - Role of Calculus and Local FactorsHeba S RadaidehNo ratings yet
- ProposalDocument5 pagesProposalapi-354921474No ratings yet
- The Effectiveness of Auxiliary Features On A Tooth Preparation With Inadequate Resistance FormDocument9 pagesThe Effectiveness of Auxiliary Features On A Tooth Preparation With Inadequate Resistance FormJhon Anderson Buendìa GarcìaNo ratings yet
- A 100-Year Journey From GV Black To Minimal Surgical InterventionDocument6 pagesA 100-Year Journey From GV Black To Minimal Surgical InterventionMichael XuNo ratings yet
- Medical Problems in DentistryDocument13 pagesMedical Problems in DentistryعصامالعبيديNo ratings yet
- Gingival EnlargementDocument125 pagesGingival Enlargementdr_saurabhsinha_165No ratings yet
- PerioDocument40 pagesPerioKavin SandhuNo ratings yet
- ACJ 2017 ProtocolDocument17 pagesACJ 2017 ProtocollkjhgfdsalkNo ratings yet
- Rationale For Scaling and Root PlaningDocument34 pagesRationale For Scaling and Root PlaningPraful ChaudhariNo ratings yet
- Krok 2 Stomatology: Test Items For Licensing ExaminationDocument30 pagesKrok 2 Stomatology: Test Items For Licensing ExaminationjimmyNo ratings yet
- 2015Document45 pages2015jimmyNo ratings yet
- MGR Univ - PerioDocument8 pagesMGR Univ - PerioMohamed FaizalNo ratings yet
- Avulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The ToothDocument39 pagesAvulsion: DEFINITION: - Tooth Avulsion (Exarticulation) Implies Total Displacement of The Toothshailesh_shenoyNo ratings yet
- Classification of Dental CariesDocument80 pagesClassification of Dental CariesOsman SoormaNo ratings yet
- Dental Considerations-CVS DiseasesDocument86 pagesDental Considerations-CVS Diseasesapi-3704106100% (1)
- Conservative QuestionsDocument4 pagesConservative QuestionsKavita GamitNo ratings yet
- 3rd BDS Oral PathologyDocument12 pages3rd BDS Oral Pathologymustafa_tambawalaNo ratings yet
- Literature GuideDocument60 pagesLiterature Guide12345sagarNo ratings yet
- Banerjee - 2018 - Selective Removal of Carious DentinDocument16 pagesBanerjee - 2018 - Selective Removal of Carious DentinAli Al-QaysiNo ratings yet
- Rationale of Periodontal TreatmentDocument5 pagesRationale of Periodontal Treatmentdileep9002392No ratings yet
- Preprosthetic Surgery 12-02-015Document32 pagesPreprosthetic Surgery 12-02-015Yaser JasNo ratings yet
- Indications For Removal of TeethDocument27 pagesIndications For Removal of TeethMoh'dMAssufiNo ratings yet
- When To Plan PFM ExtractionsDocument10 pagesWhen To Plan PFM ExtractionssarahNo ratings yet
- Denture BaseDocument59 pagesDenture BasesarahNo ratings yet
- Denture BaseDocument59 pagesDenture BasesarahNo ratings yet
- Abnormalities of Primary and Mixed DentitionDocument39 pagesAbnormalities of Primary and Mixed DentitionsarahNo ratings yet
- 1-Impression TechniquesTheoriesDocument19 pages1-Impression TechniquesTheoriessarahNo ratings yet
- Bone Tumors HODocument81 pagesBone Tumors HOOsman SoormaNo ratings yet
- Treatment Plan For Periodontal Diseases NEWDocument20 pagesTreatment Plan For Periodontal Diseases NEWsarahNo ratings yet
- Minor ConnectorsDocument61 pagesMinor Connectorssarah100% (1)
- Introduction History Examination (Prosthodontics)Document37 pagesIntroduction History Examination (Prosthodontics)sarah0% (1)
- Jaw DisorderDocument42 pagesJaw DisordersarahNo ratings yet
- ENT Lecture!Document31 pagesENT Lecture!sarahNo ratings yet
- Cleft Lip PalateDocument35 pagesCleft Lip PalatesarahNo ratings yet
- Odontomes and Odontogenic TumoursDocument16 pagesOdontomes and Odontogenic TumourssarahNo ratings yet
- Oralmed SEQDocument8 pagesOralmed SEQsarahNo ratings yet
- Cae Open Cloze PhobiasDocument3 pagesCae Open Cloze PhobiasValéria DuczaNo ratings yet
- Accreditation and Certification 10 09Document2 pagesAccreditation and Certification 10 09Snegha RajaNo ratings yet
- Pain Management Guide PDFDocument5 pagesPain Management Guide PDFPriydarshni KohliNo ratings yet
- MedsDocument2 pagesMedsRuel MaddawinNo ratings yet
- Preventive Medicine and GeriatricsDocument37 pagesPreventive Medicine and GeriatricsVicky Sankaran67% (3)
- Anaemia: by Swaathi R Final Year MbbsDocument33 pagesAnaemia: by Swaathi R Final Year MbbsGopi NathNo ratings yet
- Rehabilitation Part IDocument87 pagesRehabilitation Part IMrunali BawaskarNo ratings yet
- Survanta PiDocument10 pagesSurvanta PiBas BaylonNo ratings yet
- Tropisetron 26Document6 pagesTropisetron 26Tori SepriwanNo ratings yet
- Diagnosis & Management of NstemiDocument26 pagesDiagnosis & Management of NstemiwlshakespeareNo ratings yet
- Abdomenul AcutDocument5 pagesAbdomenul Acutcristina ovidenieNo ratings yet
- SWS Bibliography1Document3 pagesSWS Bibliography1Valaki MimiNo ratings yet
- Lifewater LatrineDesignandConstruction ManualDocument270 pagesLifewater LatrineDesignandConstruction ManualDelovan CheikhoNo ratings yet
- DR - Kavita Priya Iicm 1Document68 pagesDR - Kavita Priya Iicm 1Kavita PriyaNo ratings yet
- Indices and Measurement of Dental CariesDocument19 pagesIndices and Measurement of Dental Cariesmaher0% (1)
- K6 - Tetanus PEDIATRICDocument23 pagesK6 - Tetanus PEDIATRICbanuperiahNo ratings yet
- Dorothea Orem-Self Care TheoryDocument10 pagesDorothea Orem-Self Care TheoryNikhil MohanNo ratings yet
- Therapeutic Effects of Phytochemicals and MedicinaDocument11 pagesTherapeutic Effects of Phytochemicals and MedicinaMd. JubairNo ratings yet
- Acute Appendicitis in PregnancyDocument18 pagesAcute Appendicitis in Pregnancynicholas Rojas SIlvaNo ratings yet
- Evaluation of Passive Stretching in The Hamstrings FlexibilityDocument10 pagesEvaluation of Passive Stretching in The Hamstrings FlexibilitylinaNo ratings yet
- Punjab Drugs Rules 2007Document33 pagesPunjab Drugs Rules 2007RphNaeemMalik75% (12)