You might also like
- Chapter II - Anemia and Hypovolemic Shock Secondary To An Upper Gastrointestinal BleedingDocument3 pagesChapter II - Anemia and Hypovolemic Shock Secondary To An Upper Gastrointestinal BleedingKn VelasquezNo ratings yet
- History and Examination in Obstetrics and Gynaecology Obstetrics History - Detailed History and Examination For The Assessment of Mother and Fetus, Identify Risk Factors in Them and Plan ManagementDocument29 pagesHistory and Examination in Obstetrics and Gynaecology Obstetrics History - Detailed History and Examination For The Assessment of Mother and Fetus, Identify Risk Factors in Them and Plan ManagementÅbübâkêř Äbd-ëřhēēm BãřřîNo ratings yet
- Definition, Classification, Etiology, and Pathophysiology of Shock in Adults (UPTODATE)Document17 pagesDefinition, Classification, Etiology, and Pathophysiology of Shock in Adults (UPTODATE)Annie K.No ratings yet
- History Taking Components for Patient AssessmentDocument20 pagesHistory Taking Components for Patient AssessmentCabdisacid yasinNo ratings yet
- STEMIDocument36 pagesSTEMIYellyasta Siusiu ImranNo ratings yet
- Adult Soap Note GuideDocument5 pagesAdult Soap Note Guidelizdp21No ratings yet
- Common Procedures in Paediatric IcuDocument17 pagesCommon Procedures in Paediatric IcuNeethu Mariya MathewNo ratings yet
- Diagnosis of ShockDocument9 pagesDiagnosis of ShockRejina RavindranNo ratings yet
- Leopando Hospice-Palliative3Document2 pagesLeopando Hospice-Palliative3Judy Ignacio EclarinoNo ratings yet
- Hypertension in PregnancyDocument20 pagesHypertension in PregnancyFAMED RESIDENTS CESMED100% (1)
- Eportfolio SampleDocument46 pagesEportfolio SampleJolaine ValloNo ratings yet
- TuberculosisDocument42 pagesTuberculosisGilbertoMpakaniyeNo ratings yet
- Principals of Paediatric History Taking and Physical ExaminationDocument17 pagesPrincipals of Paediatric History Taking and Physical ExaminationKingston HoNo ratings yet
- Presented By: Henna Dhir Roll No.: RP7005A01 Regd No.: 11002446Document31 pagesPresented By: Henna Dhir Roll No.: RP7005A01 Regd No.: 11002446hennadhir2No ratings yet
- History and Physical ExaminationDocument17 pagesHistory and Physical ExaminationNur Fatima SanaaniNo ratings yet
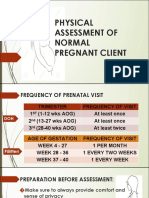
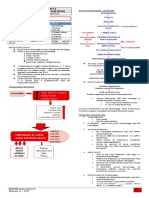
- Physical Assessment of a Pregnant ClientDocument25 pagesPhysical Assessment of a Pregnant ClientDe Leon, Austine Sydney D.No ratings yet
- Enteral Parenteral NutritionDocument80 pagesEnteral Parenteral NutritionJehangir AllamNo ratings yet
- ALD WITH ASCITES by VaibhavDocument22 pagesALD WITH ASCITES by VaibhavSandeep ChakravarthyNo ratings yet
- Pediatric Clinical ExaminationDocument37 pagesPediatric Clinical ExaminationHalema Al OkshNo ratings yet
- Junior Intern NotesDocument3 pagesJunior Intern NotesTin SumangaNo ratings yet
- 107 Rle Virtual Duty - Opd: Internal MedicineDocument6 pages107 Rle Virtual Duty - Opd: Internal MedicineGiel Margareth LindoNo ratings yet
- Tuberculosis: Therapeutics IIDocument54 pagesTuberculosis: Therapeutics IIdstu20No ratings yet
- Physician Order Sheet Format GuideDocument9 pagesPhysician Order Sheet Format GuideRoland Philip GoNo ratings yet
- Hypovolemic Shock: by DR Teh W.CDocument29 pagesHypovolemic Shock: by DR Teh W.CTeh Wai Choon100% (1)
- Patient with Eustachian Tube Dysfunction and Otitis MediaDocument5 pagesPatient with Eustachian Tube Dysfunction and Otitis MediaRenz Marion AlemaniaNo ratings yet
- Inhaler Testing BrochureDocument132 pagesInhaler Testing BrochureMathaiosVNo ratings yet
- Pediatric Tickler by RemDocument7 pagesPediatric Tickler by RemRem AlfelorNo ratings yet
- Pre-Operative Orders Post-Op Orders (Ga)Document3 pagesPre-Operative Orders Post-Op Orders (Ga)Alissandra OcampoNo ratings yet
- IM Cardiology Samplex All-In - LDocument35 pagesIM Cardiology Samplex All-In - LDeepbluexNo ratings yet
- National Guideline for Clinical Management of Dengue SyndromeDocument96 pagesNational Guideline for Clinical Management of Dengue SyndromeTapash GopeNo ratings yet
- First Line Drugs by Infection and ConditionDocument3 pagesFirst Line Drugs by Infection and ConditionKeisha Dela CernaNo ratings yet
- 19499-Enteral Parenteral NutritionDocument53 pages19499-Enteral Parenteral NutritionZunni HermawatiNo ratings yet
- Trials SummaryDocument12 pagesTrials SummaryReda SoNo ratings yet
- PEDIA ER FormularyDocument1 pagePEDIA ER FormularyAnonymous ic2CDkFNo ratings yet
- CPG PneumoniaDocument31 pagesCPG PneumoniaJo Anne100% (3)
- Carbuncle, Incision, Drainage, DebridementDocument11 pagesCarbuncle, Incision, Drainage, DebridementAlvin Germo PasuquinNo ratings yet
- TICKLER-PRINT-2 Pedia PDFDocument7 pagesTICKLER-PRINT-2 Pedia PDFCarlos H. AcuñaNo ratings yet
- Foundation Programme Curriculum 2016Document100 pagesFoundation Programme Curriculum 2016breadfanNo ratings yet
- Core Values of Family MedicineDocument68 pagesCore Values of Family MedicineJodene Rose RojasNo ratings yet
- Philippines TB CP Guidelines 2006Document151 pagesPhilippines TB CP Guidelines 2006wiltechworksNo ratings yet
- History Taking - The Critical First Step in DiagnosisDocument51 pagesHistory Taking - The Critical First Step in DiagnosisJAMES TONNY OKINYINo ratings yet
- Hypovolemic Shock & DIC (Bernabe)Document4 pagesHypovolemic Shock & DIC (Bernabe)NoreenNo ratings yet
- Action Plan PICU FINALDocument2 pagesAction Plan PICU FINALMark MacasadduNo ratings yet
- Ortho History Taking & Physical ExaminationDocument28 pagesOrtho History Taking & Physical ExaminationCabdi WaliNo ratings yet
- 1st Lecture of Respiratory Histology by DR RoomiDocument24 pages1st Lecture of Respiratory Histology by DR RoomiMudassar Roomi100% (1)
- Malaysia's National Essential Drug List 3rd Ed.Document10 pagesMalaysia's National Essential Drug List 3rd Ed.afiq83No ratings yet
- Acute Circulatory FailureDocument29 pagesAcute Circulatory FailureSanthoshi Sadhanaa SankarNo ratings yet
- Guide To The Comprehensive Pediatric H and P Write Up PDFDocument16 pagesGuide To The Comprehensive Pediatric H and P Write Up PDFnanaNo ratings yet
- TB Treatment Guidelines and Anti-Tuberculosis DrugsDocument43 pagesTB Treatment Guidelines and Anti-Tuberculosis DrugsQii ishNo ratings yet
- Emergency Drugs: Drug Action Indications Adverse Effects Contraindications Nursing Management Atropine SulfateDocument15 pagesEmergency Drugs: Drug Action Indications Adverse Effects Contraindications Nursing Management Atropine Sulfate092109No ratings yet
- Sample Three: Physician and Hospital ContractDocument12 pagesSample Three: Physician and Hospital ContractMario Lopez100% (1)
- Pedia DosesDocument7 pagesPedia DosesSai Krishna MaddiralaNo ratings yet
- PEDIATRIC HISTORY AND PHYSICAL TEMPLATEDocument3 pagesPEDIATRIC HISTORY AND PHYSICAL TEMPLATELauren GrandpreNo ratings yet
- Trinx Product Catalog 2019 ENDocument64 pagesTrinx Product Catalog 2019 ENFernando BlancoNo ratings yet
- Hap VapDocument18 pagesHap VapAgita GintingNo ratings yet
- Ioc Gold StandardDocument6 pagesIoc Gold StandardjohnNo ratings yet
- H&P GuideDocument7 pagesH&P GuideTBWPNo ratings yet
- Benefits of SMART Therapy For Asthma ManagementDocument4 pagesBenefits of SMART Therapy For Asthma ManagementREDANo ratings yet
- Asthma Control SABA UseDocument9 pagesAsthma Control SABA UsemapuxdNo ratings yet
- Effective asthma management with written action plansDocument4 pagesEffective asthma management with written action plansdarkheart1804No ratings yet
- AdultDocument295 pagesAdultKen WonNo ratings yet
- Asa PSC System PDFDocument2 pagesAsa PSC System PDFKen WonNo ratings yet
- Citizen InstructDocument18 pagesCitizen InstructKen WonNo ratings yet
- Adult Ascites EnhancedDocument96 pagesAdult Ascites EnhancedPutri Rafika ZahrahNo ratings yet
- Clerkship Handbook: Family MedicineDocument51 pagesClerkship Handbook: Family MedicineKen WonNo ratings yet
- Inter-Rater Reliability PSCDocument6 pagesInter-Rater Reliability PSCKen WonNo ratings yet
- 1 S PSCDocument8 pages1 S PSCKen WonNo ratings yet
- Transition To Practice Tips 2018Document17 pagesTransition To Practice Tips 2018Ken WonNo ratings yet
- ACLS Provider Manual Supplementary Material: © 2016 American Heart AssociationDocument74 pagesACLS Provider Manual Supplementary Material: © 2016 American Heart AssociationKen WonNo ratings yet
- Canon EOS FlashWorkDocument17 pagesCanon EOS FlashWorkKeith ClintonNo ratings yet
- I 30 I 40Document27 pagesI 30 I 40Ken WonNo ratings yet
- PHQ 9Document2 pagesPHQ 9zainasgher100% (1)
- Vineyard JohnDocument321 pagesVineyard JohnKen Won0% (1)
- Form Critical Analysis Is5Document12 pagesForm Critical Analysis Is5Ken WonNo ratings yet
- Laporan Kasus BronkopneumoniaDocument30 pagesLaporan Kasus BronkopneumoniaShifa Ali JannatinNo ratings yet
- Neonatal Air Leak Syndrome and The Role Of.3Document9 pagesNeonatal Air Leak Syndrome and The Role Of.3Claudia KosztelnikNo ratings yet
- Generi Life Physician Statement FormDocument1 pageGeneri Life Physician Statement FormVennus RacraquinNo ratings yet
- Diseases of The Bone Marrow and Blood Conditions That Can Occur When The Blood-Forming Cells in The Bone Marrow Become AbnormalDocument4 pagesDiseases of The Bone Marrow and Blood Conditions That Can Occur When The Blood-Forming Cells in The Bone Marrow Become AbnormalLuqman QadirNo ratings yet
- Coronary Artery Disease (CAD) Angina Pectoris: Chapter 28: Management of Patients With CVDDocument3 pagesCoronary Artery Disease (CAD) Angina Pectoris: Chapter 28: Management of Patients With CVDLizzy WayNo ratings yet
- Immediate Life Support - NewDocument67 pagesImmediate Life Support - NewTalhaNo ratings yet
- Birth StoryDocument2 pagesBirth Storyapi-549201461No ratings yet
- Pathophysiology: Predisposing Factors: Precipitating FactorsDocument2 pagesPathophysiology: Predisposing Factors: Precipitating FactorsJemsMei Comparativo MensuradoNo ratings yet
- PolicyDocument8 pagesPolicyjoshiaruna539No ratings yet
- Vital Signs and Monitoring - Worksheet - IntermediateDocument5 pagesVital Signs and Monitoring - Worksheet - IntermediateVadim BulbakNo ratings yet
- ECSI Instructor Update 2021Document52 pagesECSI Instructor Update 2021Zach MatthewsNo ratings yet
- List of Hospitals in Delhi NCRDocument484 pagesList of Hospitals in Delhi NCRVaibhav BahetiNo ratings yet
- Faculty of Medicine and Health Sciences Score Sheet For CASE Write-UpDocument30 pagesFaculty of Medicine and Health Sciences Score Sheet For CASE Write-UpJared Khoo Er HauNo ratings yet
- Suxamethonium Apnoea Update 2003Document2 pagesSuxamethonium Apnoea Update 2003jira neaNo ratings yet
- Treatment Plan TemplatesDocument2 pagesTreatment Plan TemplatesShalini Dass100% (3)
- Types of Insulin For Diabetes TreatmentDocument2 pagesTypes of Insulin For Diabetes TreatmentKrystale Mae ValdezNo ratings yet
- DKA Protocol With Calculation SheetDocument7 pagesDKA Protocol With Calculation SheetAmanda Marie Best OsbourneNo ratings yet
- AJEERNA (Indigestion)Document37 pagesAJEERNA (Indigestion)m gouriNo ratings yet
- Personal Hygiene Habits for Better HealthDocument1 pagePersonal Hygiene Habits for Better HealthPISMP BA2100% (1)
- Ecmo TroubleshootingDocument1 pageEcmo TroubleshootingMitch ConnerNo ratings yet
- Circulatory SystemDocument21 pagesCirculatory SystemYusuf AzeezNo ratings yet
- AIAPGET 2018 analysisDocument4 pagesAIAPGET 2018 analysisarpit sachanNo ratings yet
- Mamas ReconstruccionDocument10 pagesMamas ReconstruccionDIOGENESNo ratings yet
- Andrew Eastman Resume 3Document2 pagesAndrew Eastman Resume 3api-281509868No ratings yet
- PercocetDocument2 pagesPercocetNinoska Garcia-OrtizNo ratings yet
- CH 14 Digestive-SystemDocument179 pagesCH 14 Digestive-SystemAntonio Calleja IINo ratings yet
- Umbilical Vein CatheterizationDocument3 pagesUmbilical Vein CatheterizationrohitNo ratings yet
- Mudra TherapyDocument72 pagesMudra TherapySundarskpNo ratings yet
- 6 Cognitive Behavioral Therapy Techniques For Bipolar DisorderDocument7 pages6 Cognitive Behavioral Therapy Techniques For Bipolar Disorderprabha50% (2)
- Cheatsheet PDFDocument2 pagesCheatsheet PDFJudaeo SandovalNo ratings yet