You might also like
- Teaching Files: Detailed Newborn ExaminationDocument51 pagesTeaching Files: Detailed Newborn ExaminationcorinadumitruNo ratings yet
- Assesment of The Newborn Baby-KuliahDocument66 pagesAssesment of The Newborn Baby-KuliahDhana AstikaNo ratings yet
- Lecture 1 ApgarDocument5 pagesLecture 1 Apgarapi-264459929No ratings yet
- NEWBORN ExaminationDocument38 pagesNEWBORN ExaminationEslam HamadaNo ratings yet
- Physical Examination of The NewbornDocument39 pagesPhysical Examination of The NewbornSabita Jana100% (1)
- Newborn: Pop C. Fonghe Group 6Document71 pagesNewborn: Pop C. Fonghe Group 6Bezza Mae Roche CruzNo ratings yet
- Newborn Baby Assessment NIPE OSCE GuideDocument23 pagesNewborn Baby Assessment NIPE OSCE GuideChen BrionesNo ratings yet
- Newborn Physical ExaminationDocument4 pagesNewborn Physical ExaminationastrikusumadewiNo ratings yet
- The First Few HoursDocument8 pagesThe First Few HoursAili BellissimaNo ratings yet
- 51 Lecture The Gynecological ExamDocument69 pages51 Lecture The Gynecological ExamTarek TarekNo ratings yet
- Newborn ExaminationDocument45 pagesNewborn ExaminationHamka HamNo ratings yet
- Neonatology Lec1 2023Document17 pagesNeonatology Lec1 2023khaleelNo ratings yet
- Assessment of NeonateDocument11 pagesAssessment of NeonateAbhishek GirdharNo ratings yet
- Newborn Examination: Rafat MosalliDocument65 pagesNewborn Examination: Rafat MosallishelasuhudNo ratings yet
- Anorectal Malformations: Presented by Khushveer KaurDocument91 pagesAnorectal Malformations: Presented by Khushveer KaurKataria DavinNo ratings yet
- Assessing The Newborn and Infant-NewDocument11 pagesAssessing The Newborn and Infant-NewJan Jamison ZuluetaNo ratings yet
- 1 Students Copy HR NewbornDocument20 pages1 Students Copy HR NewbornfatimamercaNo ratings yet
- Down SyndromeDocument6 pagesDown SyndromeAnsu Maliyakal100% (1)
- OB-GYN ExaminationDocument9 pagesOB-GYN ExaminationsalmaNo ratings yet
- Newborn Examination 2015Document61 pagesNewborn Examination 2015rajanNo ratings yet
- Abnormalities Of The Testis And Scrotum: A Concise GuideDocument34 pagesAbnormalities Of The Testis And Scrotum: A Concise GuideIma MoriNo ratings yet
- Physical Examination: Presented To Mrs. Nisha Mane Assistant Professor D.Y.P.S.O.NDocument41 pagesPhysical Examination: Presented To Mrs. Nisha Mane Assistant Professor D.Y.P.S.O.NNilakshi Barik MandalNo ratings yet
- Newborn first exam and screening essentialsDocument23 pagesNewborn first exam and screening essentialsloglesb1No ratings yet
- Newborn Exam Tutorial 5Document4 pagesNewborn Exam Tutorial 5Naomi OraengNo ratings yet
- 03-First Trimester UsgDocument103 pages03-First Trimester UsgBharti Pant GahtoriNo ratings yet
- Cardiovascular (CVS) Examination: Procedure StepsDocument15 pagesCardiovascular (CVS) Examination: Procedure StepsGeorich NarcisoNo ratings yet
- Assesment of The Newborn Baby-KuliahDocument67 pagesAssesment of The Newborn Baby-Kuliahamel015No ratings yet
- Care For High Risk NewbornDocument293 pagesCare For High Risk NewbornColeen PequitNo ratings yet
- Apgar Score May Be Influenced By: Preterm Birth Administration of Maternal Drugs Congenital AnomaliesDocument36 pagesApgar Score May Be Influenced By: Preterm Birth Administration of Maternal Drugs Congenital AnomaliesZimm RrrrNo ratings yet
- Physical Exam Internal FINALDocument27 pagesPhysical Exam Internal FINALMohammad AlrefaiNo ratings yet
- Abdominal Examination DetailedDocument22 pagesAbdominal Examination Detailedsaveetha purushothamanNo ratings yet
- AssessmentDocument3 pagesAssessmentyounggirldavidNo ratings yet
- Neonatal ExaminationDocument5 pagesNeonatal ExaminationParsaant Singh100% (1)
- Newborn Physical AssessmentDocument7 pagesNewborn Physical AssessmentFady Jehad Zaben100% (1)
- Physical Assessment On AdultsDocument12 pagesPhysical Assessment On AdultsGen-GenMedranoGirayNo ratings yet
- Newborn Assessment Guide: Full Physical Exam StepsDocument23 pagesNewborn Assessment Guide: Full Physical Exam Steps.No ratings yet
- Care of The High Risk NewbornDocument309 pagesCare of The High Risk NewbornClaire Alvarez OngchuaNo ratings yet
- Guidelines On Neonatal ExaminationDocument9 pagesGuidelines On Neonatal ExaminationShitanjni WatiNo ratings yet
- Physical Exam Guide for Pediatric SurgeonsDocument7 pagesPhysical Exam Guide for Pediatric SurgeonsMuhammadRifqiFarizanAkbarNo ratings yet
- Abc Abuso 1 PDFDocument6 pagesAbc Abuso 1 PDFMDMNo ratings yet
- Thyroid Examination SchemeDocument3 pagesThyroid Examination SchemeUsman Ali AkbarNo ratings yet
- Key signs and symptoms of infantile pyloric stenosisDocument6 pagesKey signs and symptoms of infantile pyloric stenosisNeil AlviarNo ratings yet
- Pediatric Clinical ExaminationDocument37 pagesPediatric Clinical ExaminationHalema Al OkshNo ratings yet
- Lymphadenopathy: Examination ProcedureDocument9 pagesLymphadenopathy: Examination ProcedureBeenish IqbalNo ratings yet
- New Born AssessmentDocument42 pagesNew Born AssessmentBhawna Joshi100% (3)
- Assessment of A Newborn in PNC Ward: Names: Londani Tamuhla Id:201703171 Course Code: Bns402Document2 pagesAssessment of A Newborn in PNC Ward: Names: Londani Tamuhla Id:201703171 Course Code: Bns402Londani TamuhlaNo ratings yet
- Focused AssessmentDocument5 pagesFocused AssessmentPiyali SahaNo ratings yet
- Physical Examination in PaediatricsDocument162 pagesPhysical Examination in PaediatricsUsman Ali100% (1)
- Normal NewbornAssessmentDocument53 pagesNormal NewbornAssessmentMidori SanNo ratings yet
- Fetal head position during descentDocument29 pagesFetal head position during descentعمر احمد شاكرNo ratings yet
- Care of The Normal Newborn: M. Rogers-Walker, MSN/Ed, RNDocument28 pagesCare of The Normal Newborn: M. Rogers-Walker, MSN/Ed, RNyanetp01No ratings yet
- Neonate ExaminationDocument11 pagesNeonate ExaminationJana AldourNo ratings yet
- Pediatrics RemarksDocument62 pagesPediatrics RemarksGÖKSU SAYGILINo ratings yet
- Approach To Pediatric HemoptysisDocument5 pagesApproach To Pediatric HemoptysisAssma Haytham MuradNo ratings yet
- Neural tube defects, pediatricDocument8 pagesNeural tube defects, pediatricReema Akberali nooraniNo ratings yet
- Newborn Examination: Assess Growth, Vitals and Body SystemsDocument132 pagesNewborn Examination: Assess Growth, Vitals and Body SystemsdevilstNo ratings yet
- The Rabbit Consultation Part Two Clinical ExaminationDocument16 pagesThe Rabbit Consultation Part Two Clinical ExaminationVistarina YuscratesNo ratings yet
- OHNS--Otolaryngology; Head and Neck surgery: pocket field guideFrom EverandOHNS--Otolaryngology; Head and Neck surgery: pocket field guideNo ratings yet
- CNS Tumor Map 2020 FullDocument1 pageCNS Tumor Map 2020 FullAlves de MeloNo ratings yet
- Dissection Manual Karl StorzDocument80 pagesDissection Manual Karl StorzazadutNo ratings yet
- Anatomia Del TalloDocument24 pagesAnatomia Del TallofrancyNo ratings yet
- Bohl 2017Document12 pagesBohl 2017Alves de MeloNo ratings yet
- What's Here?: 5 LevelsDocument3 pagesWhat's Here?: 5 LevelsTamara Anita LimaNo ratings yet
- Operative Compared With Nonoperative Treatment of A Thoracolumbar Burst Fracture Without Neurological DeficitDocument9 pagesOperative Compared With Nonoperative Treatment of A Thoracolumbar Burst Fracture Without Neurological DeficitAlves de MeloNo ratings yet
- Protocolo HsaeDocument19 pagesProtocolo HsaeAlves de MeloNo ratings yet
- ABI D Arapiraca JVUDocument5 pagesABI D Arapiraca JVUAlves de MeloNo ratings yet
- Aula 4 - Vancouver Style How To Cite ReferencesDocument16 pagesAula 4 - Vancouver Style How To Cite ReferencesAlves de MeloNo ratings yet
- How Are You Today? What's Your Name? What Old Are You? Do You Have Any Brothers or Sisters? Where Are You From?Document12 pagesHow Are You Today? What's Your Name? What Old Are You? Do You Have Any Brothers or Sisters? Where Are You From?Alves de MeloNo ratings yet
- Rabor vs CSC - Retirement age extension disputeDocument2 pagesRabor vs CSC - Retirement age extension disputeGladys Bustria OrlinoNo ratings yet
- Demeclocycline Effective for Treating SIADHDocument4 pagesDemeclocycline Effective for Treating SIADHSally TareqNo ratings yet
- RRL - Airbag SystemDocument3 pagesRRL - Airbag Systemclarice fNo ratings yet
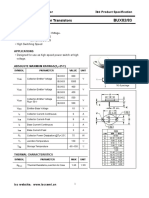
- Isc BUX82/83: Isc Silicon NPN Power TransistorsDocument2 pagesIsc BUX82/83: Isc Silicon NPN Power TransistorsCarlos HCNo ratings yet
- TuflineLinedBallValve 332148 2-07Document12 pagesTuflineLinedBallValve 332148 2-07Marcio NegraoNo ratings yet
- Sustainable City PDFDocument361 pagesSustainable City PDFagusbudiyonoNo ratings yet
- Harmonized "Cluster" Document: For Electrical Connectors Conductive Plated CoatingsDocument22 pagesHarmonized "Cluster" Document: For Electrical Connectors Conductive Plated CoatingsFrederico CésarNo ratings yet
- CIVICUS Monitoring October 2020 BriefDocument8 pagesCIVICUS Monitoring October 2020 BriefRapplerNo ratings yet
- Margaret Sanger's Role in Population Control AgendaDocument11 pagesMargaret Sanger's Role in Population Control AgendaBlackShadowSnoopy100% (1)
- Peserta Kredensial Puskesmas (Olah Data)Document15 pagesPeserta Kredensial Puskesmas (Olah Data)wahyumozabillaNo ratings yet
- The Political Ecology of Food and AgricultureDocument15 pagesThe Political Ecology of Food and AgricultureMitchNo ratings yet
- ARSA 2010 International Conference Proceeding - Volume IIDocument540 pagesARSA 2010 International Conference Proceeding - Volume IICholnapa AnukulNo ratings yet
- Aerobic BodybuilderDocument38 pagesAerobic Bodybuildercf strength80% (5)
- Siemens Arcadis Avantic Installations LaserIIDocument22 pagesSiemens Arcadis Avantic Installations LaserIINelson AltuveNo ratings yet
- CHN 2 Module 6Document11 pagesCHN 2 Module 6Carlos CerdeñaNo ratings yet
- Processing Cacao Pod Husk into Low-Methoxyl PectinDocument9 pagesProcessing Cacao Pod Husk into Low-Methoxyl PectinEmmanuel PlazaNo ratings yet
- Dissolvine 100-S MSDSDocument8 pagesDissolvine 100-S MSDSMichaelNo ratings yet
- Myth and Folklo-WPS OfficeDocument211 pagesMyth and Folklo-WPS OfficeAryan A100% (1)
- Medical Student Amnesia USMLE Step 1 - Flash Cards by CueFlashDocument13 pagesMedical Student Amnesia USMLE Step 1 - Flash Cards by CueFlashMuhammad Farhan KhaliqNo ratings yet
- SWOT Analysis AuchanDocument2 pagesSWOT Analysis AuchanDaniela DogaruNo ratings yet
- Bio Brain Review Q S PDFDocument22 pagesBio Brain Review Q S PDFtehilashiftehNo ratings yet
- Rotex Brochure PDFDocument4 pagesRotex Brochure PDFestramilsolutionNo ratings yet
- Rock CycleDocument30 pagesRock CycleDenny PrawiraNo ratings yet
- Mass XL Workout Plan by Guru Mann PDFDocument4 pagesMass XL Workout Plan by Guru Mann PDFSaptarshi BiswasNo ratings yet
- Overlooked Women in Jails Report WebDocument48 pagesOverlooked Women in Jails Report Webvanessa langaNo ratings yet
- Jim106 Chapter 1 Practice ExercisesDocument3 pagesJim106 Chapter 1 Practice ExercisesHor KaiNo ratings yet
- Categories of AnalysisDocument4 pagesCategories of AnalysisTee JackNo ratings yet
- Type I Diabetes Mellitus Management in The Athletic PopulationDocument22 pagesType I Diabetes Mellitus Management in The Athletic PopulationRitesh NetamNo ratings yet
- Capstone PresentationDocument19 pagesCapstone PresentationArun BalachandranNo ratings yet
- Public Safety BriefingDocument23 pagesPublic Safety BriefingHNNNo ratings yet