You might also like
- N.Y. Downtown Revitalization Initiative Round Five GuidebookDocument38 pagesN.Y. Downtown Revitalization Initiative Round Five GuidebookRiverheadLOCALNo ratings yet
- RXR/GGV Qualified & Eligible Documents (Final 09.26.22)Document23 pagesRXR/GGV Qualified & Eligible Documents (Final 09.26.22)RiverheadLOCALNo ratings yet
- 5-10-2022 Budget Hearing Presentation UpdatedDocument12 pages5-10-2022 Budget Hearing Presentation UpdatedRiverheadLOCALNo ratings yet
- Draft Scope Riverhead Logistics CenterDocument20 pagesDraft Scope Riverhead Logistics CenterRiverheadLOCALNo ratings yet
- Riverhead Budget Presentation March 22, 2022Document14 pagesRiverhead Budget Presentation March 22, 2022RiverheadLOCALNo ratings yet
- Riverhead Town Proposed Battery Energy Storage CodeDocument10 pagesRiverhead Town Proposed Battery Energy Storage CodeRiverheadLOCALNo ratings yet
- Yvette AguiarDocument10 pagesYvette AguiarRiverheadLOCALNo ratings yet
- Riverhead Comprehensive Plan Update Public Outreach Compendium Feb 16, 2022Document7 pagesRiverhead Comprehensive Plan Update Public Outreach Compendium Feb 16, 2022RiverheadLOCALNo ratings yet
- 2022 - 03 - 16 - EPCAL Resolution & Letter AgreementDocument9 pages2022 - 03 - 16 - EPCAL Resolution & Letter AgreementRiverheadLOCALNo ratings yet
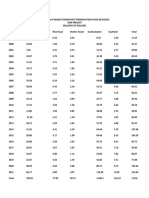
- Peconic Bay Region Community Preservation Fund Revenues 1999-2021Document1 pagePeconic Bay Region Community Preservation Fund Revenues 1999-2021RiverheadLOCALNo ratings yet
- Riverhead Town Board Comprehensive Plan Status Discussion Feb. 17, 2022Document30 pagesRiverhead Town Board Comprehensive Plan Status Discussion Feb. 17, 2022RiverheadLOCALNo ratings yet
- Riverhead Town Police Report, August 2021Document6 pagesRiverhead Town Police Report, August 2021RiverheadLOCALNo ratings yet
- AKRF Public Outreach Report AttachmentsDocument126 pagesAKRF Public Outreach Report AttachmentsRiverheadLOCALNo ratings yet
- Pediatric Covid-19 Hospitalization ReportDocument15 pagesPediatric Covid-19 Hospitalization ReportKevin TamponeNo ratings yet
- Riverhead Town Police Monthly Report July 2021Document6 pagesRiverhead Town Police Monthly Report July 2021RiverheadLOCALNo ratings yet
- Kenneth RothwellDocument5 pagesKenneth RothwellRiverheadLOCALNo ratings yet
- Catherine KentDocument7 pagesCatherine KentRiverheadLOCALNo ratings yet
- 2021 General Election - Suffolk County Sample Ballot BookletDocument154 pages2021 General Election - Suffolk County Sample Ballot BookletRiverheadLOCALNo ratings yet
- Evelyn Hobson-Womack Campaign Finance DisclosureDocument3 pagesEvelyn Hobson-Womack Campaign Finance DisclosureRiverheadLOCALNo ratings yet
- Juan Micieli-MartinezDocument3 pagesJuan Micieli-MartinezRiverheadLOCALNo ratings yet
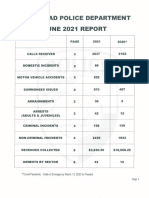
- Riverhead Town Police Monthly Report, June 2021Document6 pagesRiverhead Town Police Monthly Report, June 2021RiverheadLOCALNo ratings yet
- Riverhead Town Police Report, March 2021Document6 pagesRiverhead Town Police Report, March 2021RiverheadLOCALNo ratings yet
- Riverhead Town Police Report, January 2021Document6 pagesRiverhead Town Police Report, January 2021RiverheadLOCALNo ratings yet
- Robert E. KernDocument3 pagesRobert E. KernRiverheadLOCALNo ratings yet
- League of Women Voters of NYS 2021 Voters Guide: Ballot PropositionsDocument2 pagesLeague of Women Voters of NYS 2021 Voters Guide: Ballot PropositionsRiverheadLOCAL67% (3)
- Old Steeple Church Time CapsuleDocument4 pagesOld Steeple Church Time CapsuleRiverheadLOCALNo ratings yet
- Aguiar-Kent Campaign Finance Report 32-Day Pre GeneralDocument2 pagesAguiar-Kent Campaign Finance Report 32-Day Pre GeneralRiverheadLOCALNo ratings yet
- Navy Environmental Concerns Survey For CalvertonDocument3 pagesNavy Environmental Concerns Survey For CalvertonRiverheadLOCALNo ratings yet
- NYSED Health and Safety Guide For The 2021 2022 School YearDocument21 pagesNYSED Health and Safety Guide For The 2021 2022 School YearNewsChannel 9100% (2)
- "The Case of The DIsappering Landfill, or To Mine or Not To Mine" by Carl E. Fritz JR., PEDocument10 pages"The Case of The DIsappering Landfill, or To Mine or Not To Mine" by Carl E. Fritz JR., PERiverheadLOCALNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Introduction Definition: Types of PacemakersDocument8 pagesIntroduction Definition: Types of PacemakersPrasann RoyNo ratings yet
- NYCDEP 2007 503 Annual ReportDocument584 pagesNYCDEP 2007 503 Annual ReportNYC SludgeNo ratings yet
- Hijamah (Cupping)Document18 pagesHijamah (Cupping)Nabeel HassanNo ratings yet
- Diabetes Mellitus Complicated PregnancyDocument21 pagesDiabetes Mellitus Complicated PregnancyanojanNo ratings yet
- 1.7 Right Person, Right Place, Right Time PDFDocument3 pages1.7 Right Person, Right Place, Right Time PDFKaren Osorio GilardiNo ratings yet
- Hypokalemic Periodic ParalysisDocument2 pagesHypokalemic Periodic ParalysissakuraleeshaoranNo ratings yet
- What Is Medical DeontologyDocument11 pagesWhat Is Medical DeontologyExorticNo ratings yet
- Radiology X-Rayfilm ScreensDocument39 pagesRadiology X-Rayfilm ScreensFourthMolar.comNo ratings yet
- Peritoneal Dialysis Brochure US 401067001 A PDFDocument6 pagesPeritoneal Dialysis Brochure US 401067001 A PDFstaryk0% (1)
- Tropocells 4 Pages PDF Format January 2011Document4 pagesTropocells 4 Pages PDF Format January 2011robertoblumandradeNo ratings yet
- TM S Fusion Device Trabecular Metal Technology Cervical Solutions Surgical Technique GuideDocument24 pagesTM S Fusion Device Trabecular Metal Technology Cervical Solutions Surgical Technique GuideTiến Khổng MinhNo ratings yet
- Week 5 - Dance Safety Protocols & Emergency Resources Dancing - Preventing InjuryDocument4 pagesWeek 5 - Dance Safety Protocols & Emergency Resources Dancing - Preventing InjuryAlbert LagundayNo ratings yet
- 365 STRONG Eat Like A BodybuilderDocument10 pages365 STRONG Eat Like A BodybuilderSlevin_KNo ratings yet
- Fibula Stress Fractures: A Treatment Review: Iftach Hetsroni, MD, and Gideon Mann, MDDocument3 pagesFibula Stress Fractures: A Treatment Review: Iftach Hetsroni, MD, and Gideon Mann, MDJamaluddin HaikhahNo ratings yet
- 06 Senior Citizen PolicyDocument26 pages06 Senior Citizen PolicyJaimson FrancisNo ratings yet
- Situation 2Document8 pagesSituation 2Rodessa Mandac TarolNo ratings yet
- Cae Open Cloze PhobiasDocument3 pagesCae Open Cloze PhobiasValéria DuczaNo ratings yet
- Theory Application 4.2.10Document80 pagesTheory Application 4.2.10shoba088083% (6)
- Youstina Khalaf Exam 26-5Document6 pagesYoustina Khalaf Exam 26-5M Usman KhanNo ratings yet
- Perdev ReviewerDocument9 pagesPerdev ReviewerPretut VillamorNo ratings yet
- Byssinosis PDFDocument8 pagesByssinosis PDFFaza AlhinduwanNo ratings yet
- Diagnosis & Management of NstemiDocument26 pagesDiagnosis & Management of NstemiwlshakespeareNo ratings yet
- Manganese DioxideDocument5 pagesManganese Dioxidemartinusteddy2114No ratings yet
- Termimesh TMA 725 MSDS January 2015Document5 pagesTermimesh TMA 725 MSDS January 2015sschkadeNo ratings yet
- Neem TreeDocument4 pagesNeem Treedorzky22No ratings yet
- ASCCP Management Guidelines - August 2014 PDFDocument24 pagesASCCP Management Guidelines - August 2014 PDFAnita BlazevskaNo ratings yet
- Don Mottin - Stage Hypnosis - Class HandoutsDocument46 pagesDon Mottin - Stage Hypnosis - Class HandoutsRaphael Maurin100% (2)
- Myles Textbook For Midwives, 15th Edition: Journal of Obstetrics and GynaecologyDocument3 pagesMyles Textbook For Midwives, 15th Edition: Journal of Obstetrics and Gynaecologyintan wahyuNo ratings yet
- Kevin Chen - Book Review: Scientific Qigong Exploration: The Wonders and Mysteries of Qi by Lu, ZuyinDocument6 pagesKevin Chen - Book Review: Scientific Qigong Exploration: The Wonders and Mysteries of Qi by Lu, ZuyinSonyRedNo ratings yet
- Tropisetron 26Document6 pagesTropisetron 26Tori SepriwanNo ratings yet