You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Transcript - FSM and The Virus Webinar - March 2020Document36 pagesTranscript - FSM and The Virus Webinar - March 2020dheenadayalanNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- WHO 2019 NCoV SARI Toolkit 2022.1 EngDocument306 pagesWHO 2019 NCoV SARI Toolkit 2022.1 EngMuhammadAgungNugrohoNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Covid 19 Notifiable PIDsr PDFDocument73 pagesCovid 19 Notifiable PIDsr PDFjheanniver nabloNo ratings yet
- IRR RA 11332 (Revised 2020) Mandatory Reporting of Notifiable Diseases and Health Events of Public Health Concern Act (08-27)Document99 pagesIRR RA 11332 (Revised 2020) Mandatory Reporting of Notifiable Diseases and Health Events of Public Health Concern Act (08-27)Leah Rose Figueroa Paras100% (2)
- TC Record PDFDocument17 pagesTC Record PDFPeter MuennigNo ratings yet
- JHCPU Star PDFDocument12 pagesJHCPU Star PDFPeter MuennigNo ratings yet
- AJPH Muennig Neidell Perry PDFDocument7 pagesAJPH Muennig Neidell Perry PDFPeter MuennigNo ratings yet
- Tobin Montessori PDFDocument12 pagesTobin Montessori PDFPeter MuennigNo ratings yet
- SSM Pre K Policies and Health PDFDocument8 pagesSSM Pre K Policies and Health PDFPeter MuennigNo ratings yet
- Social Entr CICE PDFDocument10 pagesSocial Entr CICE PDFPeter MuennigNo ratings yet
- Tal and Sherry PDFDocument9 pagesTal and Sherry PDFPeter MuennigNo ratings yet
- Postsecondary CEA PDFDocument7 pagesPostsecondary CEA PDFPeter MuennigNo ratings yet
- Abc PDFDocument5 pagesAbc PDFPeter MuennigNo ratings yet
- Proofreading Marks PDFDocument1 pageProofreading Marks PDFPeter MuennigNo ratings yet
- Muenning&Su PDFDocument10 pagesMuenning&Su PDFPeter MuennigNo ratings yet
- Social Entrepreneurs and Education PDFDocument8 pagesSocial Entrepreneurs and Education PDFPeter MuennigNo ratings yet
- Motor Vehical Crash - PH Failure2014 PDFDocument4 pagesMotor Vehical Crash - PH Failure2014 PDFPeter MuennigNo ratings yet
- Predictors Myanmar PDFDocument6 pagesPredictors Myanmar PDFPeter MuennigNo ratings yet
- All4Ed PDFDocument7 pagesAll4Ed PDFPeter MuennigNo ratings yet
- Leven Belfield Muennig Rouse Economics of Ed Review PDFDocument10 pagesLeven Belfield Muennig Rouse Economics of Ed Review PDFPeter MuennigNo ratings yet
- Education Final Report PDFDocument26 pagesEducation Final Report PDFPeter MuennigNo ratings yet
- Well and Well-Off:: Decreasing Medicaid and Health-Care Costs by Increasing Educational AttainmentDocument11 pagesWell and Well-Off:: Decreasing Medicaid and Health-Care Costs by Increasing Educational AttainmentPeter MuennigNo ratings yet
- AJPH Education Small Class SizeDocument8 pagesAJPH Education Small Class SizePeter MuennigNo ratings yet
- 33 HPU272 Friedman PDFDocument22 pages33 HPU272 Friedman PDFPeter MuennigNo ratings yet
- Black Males PDFDocument11 pagesBlack Males PDFPeter MuennigNo ratings yet
- Well and Well-Off:: Decreasing Medicaid and Health-Care Costs by Increasing Educational AttainmentDocument11 pagesWell and Well-Off:: Decreasing Medicaid and Health-Care Costs by Increasing Educational AttainmentPeter MuennigNo ratings yet
- Welfare CEA PDFDocument5 pagesWelfare CEA PDFPeter MuennigNo ratings yet
- Using The YHL To Calculate QALYs PDFDocument5 pagesUsing The YHL To Calculate QALYs PDFPeter MuennigNo ratings yet
- AJPH Woolf StudentsDocument9 pagesAJPH Woolf StudentsPeter MuennigNo ratings yet
- AJE Class SizeDocument7 pagesAJE Class SizePeter MuennigNo ratings yet
- TB Cea Nejm PDFDocument10 pagesTB Cea Nejm PDFPeter MuennigNo ratings yet
- Health Insurance CEA PDFDocument6 pagesHealth Insurance CEA PDFPeter MuennigNo ratings yet
- The Economic Cost of Community-Based Interventions To Improve Breast Cancer Control PDFDocument12 pagesThe Economic Cost of Community-Based Interventions To Improve Breast Cancer Control PDFPeter MuennigNo ratings yet
- Kaisa Study Final Paper Super FinalDocument114 pagesKaisa Study Final Paper Super FinalEunice RiveraNo ratings yet
- WHO 2019 nCoV SurveillanceGuidance 2022.2 EngDocument33 pagesWHO 2019 nCoV SurveillanceGuidance 2022.2 EngArwa HussienNo ratings yet
- Sample Id: Sample Id: 6284347 Icmr Specimen Referral Form Icmr Specimen Referral Form For For Covid-19 (Sars-Cov2) Covid-19 (Sars-Cov2)Document2 pagesSample Id: Sample Id: 6284347 Icmr Specimen Referral Form Icmr Specimen Referral Form For For Covid-19 (Sars-Cov2) Covid-19 (Sars-Cov2)Praveen KumarNo ratings yet
- 1 s2.0 S0399077X20301104 MainDocument4 pages1 s2.0 S0399077X20301104 MainNaira ValentinaNo ratings yet
- 2 5292165759038916094 PDFDocument11 pages2 5292165759038916094 PDFSiaNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)ShakirShafiNo ratings yet
- Suffield Public Schools: Pandemic Plan 2020Document16 pagesSuffield Public Schools: Pandemic Plan 2020Jimmellee EllenNo ratings yet
- Mask Use, Hand Hygiene, and Seasonal Influenza-Like Illness Among Young Adults: A Randomized Intervention TrialDocument8 pagesMask Use, Hand Hygiene, and Seasonal Influenza-Like Illness Among Young Adults: A Randomized Intervention TrialDzulfathil PuteraNo ratings yet
- Know The Difference Between Cold and Swine Flu Symptoms Symptom Cold Swine FluDocument57 pagesKnow The Difference Between Cold and Swine Flu Symptoms Symptom Cold Swine FlususantalbriperNo ratings yet
- Name: Chintiya Cahaya Putri NIM: P20637020008 Class: 1A Prodi: Diii RmikDocument37 pagesName: Chintiya Cahaya Putri NIM: P20637020008 Class: 1A Prodi: Diii RmikChintiya PutriNo ratings yet
- Ordinance On Contact TracingDocument9 pagesOrdinance On Contact Tracingkayo roi dielNo ratings yet
- Swine FluDocument14 pagesSwine FluGovind PrasadNo ratings yet
- Rapport Annuel Santé EuropéenDocument248 pagesRapport Annuel Santé EuropéennouvelobsNo ratings yet
- Covid in PregnancyDocument30 pagesCovid in Pregnancyvidhi chaudharyNo ratings yet
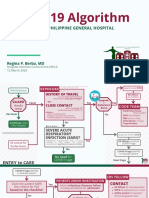
- COVID-19 Algorithm: For The Philippine General HospitalDocument10 pagesCOVID-19 Algorithm: For The Philippine General HospitalJay VeeNo ratings yet
- Integrated Health Information Platform: Integrated Disease Surveillance ProgrammeDocument6 pagesIntegrated Health Information Platform: Integrated Disease Surveillance ProgrammeSumit PatelNo ratings yet
- Covid 19 PDFDocument117 pagesCovid 19 PDFvicky anandNo ratings yet
- National Preparedness and Response Plan For Outbreak of Novel Coronavirus (COVID-19)Document45 pagesNational Preparedness and Response Plan For Outbreak of Novel Coronavirus (COVID-19)MAHARSHI SHUKLA100% (1)
- The Epidemiological Landscape of The National Influenza Sentinel Surveillance System From 2016 To 2019, TanzaniaDocument10 pagesThe Epidemiological Landscape of The National Influenza Sentinel Surveillance System From 2016 To 2019, TanzaniaInternational Journal of Innovative Science and Research Technology100% (1)
- 2021-08-01 To 2021-08-04Document822 pages2021-08-01 To 2021-08-04Gov. Ganeral Hospital putturNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)Document2 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : (If Yes, Attach Prescription If No, Test Cannot Be Conducted)narayanasmrithiNo ratings yet
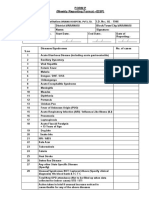
- Form P (Weekly Reporting Format - IDSP) : Oriana Hospital PVT - LTDDocument2 pagesForm P (Weekly Reporting Format - IDSP) : Oriana Hospital PVT - LTDRavi ParmarNo ratings yet
- Health Q3 M2Document15 pagesHealth Q3 M2olameonfrixandrei486No ratings yet
- Visitor/Contractor Health Declaration Form ORM: Questions Circle AnswerDocument2 pagesVisitor/Contractor Health Declaration Form ORM: Questions Circle AnswerLea CardinezNo ratings yet
- Virus Influenza Guidlines PDFDocument47 pagesVirus Influenza Guidlines PDFМарија СерафимовскаNo ratings yet
- Acute Respiratory Infections Daryl Joel Dumdum, M.DDocument5 pagesAcute Respiratory Infections Daryl Joel Dumdum, M.DJoan LuisNo ratings yet