You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Methods and Advances in Metabolic Flux Analysis: A Mini ReviewDocument9 pagesMethods and Advances in Metabolic Flux Analysis: A Mini ReviewAmal ..No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Lec 32Document24 pagesLec 32Amal ..No ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Chemical Reaction Engineering (CRE) Is TheDocument22 pagesChemical Reaction Engineering (CRE) Is TheAmal ..No ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Critical Illness: Your Companion in Critical TimesDocument2 pagesCritical Illness: Your Companion in Critical TimesAmal ..No ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Preparation of PigmentDocument3 pagesPreparation of PigmentAmal ..No ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- 7.7 Flame Arresters, Conservation Vents, and Emergency VentsDocument8 pages7.7 Flame Arresters, Conservation Vents, and Emergency VentsAmal ..No ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Apj Abdul Kalam Technological University Thiruvananthapuram, Kerala, INDIADocument26 pagesApj Abdul Kalam Technological University Thiruvananthapuram, Kerala, INDIAAmal ..No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Nptel: Process Control and Instrumentation - Web CourseDocument4 pagesNptel: Process Control and Instrumentation - Web CourseAmal ..No ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Co 2 Recovery ProcessDocument5 pagesCo 2 Recovery ProcessAmal ..No ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- To Chemical Engineer ProfessionDocument39 pagesTo Chemical Engineer ProfessionAmal ..No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Gujarat Technological UniversityDocument2 pagesGujarat Technological UniversityAmal ..No ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- 477306S Introduction Non-Ideal Reactors PDFDocument13 pages477306S Introduction Non-Ideal Reactors PDFAmal ..No ratings yet
- Type KDocument4 pagesType KAmal ..No ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Note Number 1 Examples of FRX Applications For DemonstrationDocument3 pagesNote Number 1 Examples of FRX Applications For DemonstrationAmal ..No ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Lab 8 - Biodiesel PDFDocument3 pagesLab 8 - Biodiesel PDFAmal ..No ratings yet
- S14 - Additive ManufactoringDocument21 pagesS14 - Additive ManufactoringAmal ..No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Research Proposal PDFDocument1 pageResearch Proposal PDFAmal ..No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Udf Wall TempDocument7 pagesUdf Wall TempAmal ..No ratings yet
- Qut Grading SystemDocument4 pagesQut Grading SystemAmal ..No ratings yet
- 10.1021@cen 09409 Buscon008Document1 page10.1021@cen 09409 Buscon008Amal ..No ratings yet
- LHR FEU Report 2019 Q3Document30 pagesLHR FEU Report 2019 Q3Dave1504No ratings yet
- Exhibit O-3Document19 pagesExhibit O-3徐天生No ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Extra 330Lx: U.S.Information ManualDocument284 pagesExtra 330Lx: U.S.Information ManualGourav DasNo ratings yet
- Expedition 4 Press KitDocument52 pagesExpedition 4 Press KitBob AndrepontNo ratings yet
- X GuardDocument2 pagesX GuardManuel SolisNo ratings yet
- Selection and Sizing of Control Valves For Natural Gas PDFDocument3 pagesSelection and Sizing of Control Valves For Natural Gas PDFMalouk CheniouniNo ratings yet
- The Lean Journey at The Boeing CoDocument32 pagesThe Lean Journey at The Boeing CoSteransko100% (1)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Chapter 21 - CNS-ATMDocument4 pagesChapter 21 - CNS-ATMEl Shazly SaidNo ratings yet
- Celebi NasDocument33 pagesCelebi NasSohel Ali KhanNo ratings yet
- Ica44 1 PDFDocument68 pagesIca44 1 PDFevanNo ratings yet
- Aviator90 Episode 5: Man: (0:31) Welcome Back To Another Masterful Episode of Aviator 90 From Angle ofDocument3 pagesAviator90 Episode 5: Man: (0:31) Welcome Back To Another Masterful Episode of Aviator 90 From Angle ofSergio VelasquezNo ratings yet
- Osds Omr SheetDocument412 pagesOsds Omr SheetAnil kumarNo ratings yet
- Hof 8Document106 pagesHof 8Lavern SipinNo ratings yet
- What Is SpeedDocument5 pagesWhat Is SpeedPrem PiriyahNo ratings yet
- FinalrepoDocument123 pagesFinalrepoDivya ChopraNo ratings yet
- Life & Times of The Avro Vulcan V10 December 2009Document31 pagesLife & Times of The Avro Vulcan V10 December 2009scribd2162No ratings yet
- Optimization and Fabrication of B C and Aloe Vera Reinforced Aluminium-Matrix-CompositeDocument13 pagesOptimization and Fabrication of B C and Aloe Vera Reinforced Aluminium-Matrix-CompositeHaider SyedNo ratings yet
- Vintage Airplane - Dec 2004Document36 pagesVintage Airplane - Dec 2004Aviation/Space History LibraryNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- CAA CAP739 - Flight Data MonitoringDocument191 pagesCAA CAP739 - Flight Data MonitoringHarry Nuryanto100% (1)
- Moonwalk 1.5Document1 pageMoonwalk 1.5eshachoukseNo ratings yet
- Problems-2 4012 PDFDocument5 pagesProblems-2 4012 PDFjonthemes100% (1)
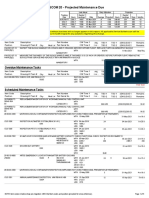
- CESCOM 20 - Projected Maintenance Due: New Requirements/Action ItemsDocument5 pagesCESCOM 20 - Projected Maintenance Due: New Requirements/Action ItemsAndré CarneiroNo ratings yet
- Cabin-Pressure Control System: Effectivity:AllDocument24 pagesCabin-Pressure Control System: Effectivity:AllclebersjcNo ratings yet
- FAR 145 Inspection SystemDocument44 pagesFAR 145 Inspection SystemFauzie Ahmad100% (1)
- Tejas Rafale Sukhoi 30 PDFDocument2 pagesTejas Rafale Sukhoi 30 PDFPahadi BhulaNo ratings yet
- Physics Key FormulasDocument4 pagesPhysics Key FormulasChidi BenedictNo ratings yet
- Principles For Pushbuttons With Integrated Indications: Pressed in On, Auto, Ovrd, Open Released Out OFF, MAN, ALTN, SHUTDocument4 pagesPrinciples For Pushbuttons With Integrated Indications: Pressed in On, Auto, Ovrd, Open Released Out OFF, MAN, ALTN, SHUTroyalairmaroc737No ratings yet
- CFD Training ManualDocument43 pagesCFD Training Manualgajendra2010No ratings yet
- 170620191KAW3B3CPFRDocument245 pages170620191KAW3B3CPFRAr Ayoushika AbrolNo ratings yet
- Aviation English Language Proficiency - Training, Test and CertificationDocument12 pagesAviation English Language Proficiency - Training, Test and CertificationDEBABRATA KAR100% (1)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 4.5 out of 5 stars4.5/5 (82)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (35)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (4)