You might also like
- 5740 11650 5 PBDocument6 pages5740 11650 5 PBdianNo ratings yet
- StresDocument5 pagesStresmuhammadfahmanNo ratings yet
- Nej Mo A 1412981Document10 pagesNej Mo A 1412981dimasNo ratings yet
- Penyakit PerdarahanDocument22 pagesPenyakit PerdarahanmuhammadfahmanNo ratings yet
- TempleteDocument10 pagesTempletemuhammadfahmanNo ratings yet
- Penda Hulu AnDocument5 pagesPenda Hulu AnmuhammadfahmanNo ratings yet
- Regional Anesthesia: Pembimbing: Dr. Dewa, Span Oleh: Annisa Aulia WidyantiDocument22 pagesRegional Anesthesia: Pembimbing: Dr. Dewa, Span Oleh: Annisa Aulia WidyantimuhammadfahmanNo ratings yet
- Journal PDFDocument6 pagesJournal PDFmuhammadfahmanNo ratings yet
- Mendel Law: Autosomal RecessiveDocument11 pagesMendel Law: Autosomal RecessivemuhammadfahmanNo ratings yet
- 01disorders of LashesDocument8 pages01disorders of LashesmuhammadfahmanNo ratings yet
- ps52 2015 Guidelines For Transport of Critically Ill Patients PDFDocument12 pagesps52 2015 Guidelines For Transport of Critically Ill Patients PDFPalwasha MalikNo ratings yet
- PBD in Pediatric AchalasiaDocument6 pagesPBD in Pediatric AchalasiamuhammadfahmanNo ratings yet
- AdhdDocument15 pagesAdhdmuhammadfahmanNo ratings yet
- Health20100800019 58835574 PDFDocument6 pagesHealth20100800019 58835574 PDFmuhammadfahmanNo ratings yet
- TromboflebitisDocument4 pagesTromboflebitismuhammadfahmanNo ratings yet
- GerdDocument12 pagesGerdcrystalastNo ratings yet
- Diagnosis, Treatment, and Prevention of Typhoid Fever (WHO)Document48 pagesDiagnosis, Treatment, and Prevention of Typhoid Fever (WHO)Nina KharimaNo ratings yet
- TifoidDocument15 pagesTifoidmuhammadfahmanNo ratings yet
- Ludwig AnginaDocument7 pagesLudwig AnginaCak BasitNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Droplet Infection: Tuberkulosis (TB) ParuDocument2 pagesDroplet Infection: Tuberkulosis (TB) ParuMiiniieNo ratings yet
- Antibiotics ResistanceDocument8 pagesAntibiotics ResistanceboredtarteelNo ratings yet
- Research Paper PneumoniaDocument7 pagesResearch Paper Pneumoniawkzcoprhf100% (1)
- Parasitic Diseases of The LungDocument27 pagesParasitic Diseases of The Lungsultan khabeebNo ratings yet
- Meningococcemia: Neisseria Meningitidis - Is An EncapsulatedDocument19 pagesMeningococcemia: Neisseria Meningitidis - Is An EncapsulatedcarolinecayasaNo ratings yet
- Report ViewerDocument1 pageReport ViewerZeeshan JunejoNo ratings yet
- Aloe Vera EthanolicextractsofaloeveraDocument8 pagesAloe Vera EthanolicextractsofaloeveraBashaar HamdaanNo ratings yet
- Test Report: Naso and Oropharyngeal SwabDocument2 pagesTest Report: Naso and Oropharyngeal SwabSanjay ThakkarNo ratings yet
- ChromAgar Brochure BDDocument16 pagesChromAgar Brochure BDapi-3697331100% (1)
- Deterministic Malaria Transmission Model With Acquired ImmunityDocument6 pagesDeterministic Malaria Transmission Model With Acquired ImmunityAchmad Nur AlphiantoNo ratings yet
- National Service Training Program: "Reaction Paper"Document4 pagesNational Service Training Program: "Reaction Paper"Stefanny Anne GuminangNo ratings yet
- Fever With Rash in Table Form.Document4 pagesFever With Rash in Table Form.Azizan HannyNo ratings yet
- Coronavirus (COVID-19) : Protocols To Mitigate The Risks of Cases On Board ShipsDocument7 pagesCoronavirus (COVID-19) : Protocols To Mitigate The Risks of Cases On Board ShipsAnand RamanNo ratings yet
- CandidiasisDocument6 pagesCandidiasisNabrazz SthaNo ratings yet
- The Role of Useful Microorganism and Harmful EffectsDocument8 pagesThe Role of Useful Microorganism and Harmful EffectswaidabNo ratings yet
- Condom Use and Associated Factors Among Hiv PDFDocument114 pagesCondom Use and Associated Factors Among Hiv PDFBuleloNo ratings yet
- CDC - Pelvic Inflammatory Disease - 2010 STD Treatment GuidelinesDocument7 pagesCDC - Pelvic Inflammatory Disease - 2010 STD Treatment GuidelinesAhmad Arbi AninditoNo ratings yet
- Microbial Diseases of The Respiratory SystemDocument30 pagesMicrobial Diseases of The Respiratory SystemChristopher Eria Santiañez0% (1)
- Chikungunya Fever Presentation For Health PractitionersDocument27 pagesChikungunya Fever Presentation For Health PractitionersPrimasari DiahNo ratings yet
- Parasitology at GlanceDocument6 pagesParasitology at GlanceRinkalNo ratings yet
- ENG - SE SATGAS COVID NO 1 - 2023 - FinalDocument4 pagesENG - SE SATGAS COVID NO 1 - 2023 - FinalLusi FadilahNo ratings yet
- Hiv AidsDocument2 pagesHiv AidsAyyue 28No ratings yet
- Handbook of Poultry DiseasesDocument22 pagesHandbook of Poultry DiseasesSoufian CherkiNo ratings yet
- Operational Guidelines On Limited Face To Face ImplementationDocument36 pagesOperational Guidelines On Limited Face To Face ImplementationJohn Paul light100% (3)
- Maklumat Vaksinasi: Vaccination DetailsDocument2 pagesMaklumat Vaksinasi: Vaccination DetailsHazadiana ZainalNo ratings yet
- Budget of Work in Health Grade 8Document2 pagesBudget of Work in Health Grade 8Jobilee MayNo ratings yet
- Immunologic Study of StreptolysinDocument12 pagesImmunologic Study of StreptolysinAishwarya BharathNo ratings yet
- Tarifario Referencia 2021 Higuera Actualizado SeptiembreDocument82 pagesTarifario Referencia 2021 Higuera Actualizado SeptiembreKariiiNo ratings yet
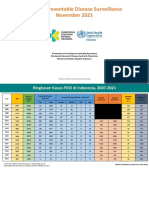
- 11 - VPD Surveillance Performance Analysis 2021 November 2021 (29122021)Document57 pages11 - VPD Surveillance Performance Analysis 2021 November 2021 (29122021)Kiky RizkyNo ratings yet
- Arbovirus EpidemiologyDocument48 pagesArbovirus EpidemiologyEdward ChavezNo ratings yet