You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Difference CD Allergic With IrritantDocument1 pageDifference CD Allergic With IrritantIsnaNo ratings yet
- Hemorrhoids-Staples vs. FergusonDocument13 pagesHemorrhoids-Staples vs. FergusonIsnaNo ratings yet
- Interna - Jurnal 1 - Isnati Rahayu 2012730053Document58 pagesInterna - Jurnal 1 - Isnati Rahayu 2012730053IsnaNo ratings yet
- Childhood AsthmaDocument9 pagesChildhood Asthmanaufal12345No ratings yet
- Kronik Rinosinusitis 6 Hal PDFDocument6 pagesKronik Rinosinusitis 6 Hal PDFIsnaNo ratings yet
- Child Abuse Inventory at Emergency Rooms: CHAIN-ER Rationale and DesignDocument7 pagesChild Abuse Inventory at Emergency Rooms: CHAIN-ER Rationale and DesignIsnaNo ratings yet
- Morpot Interna 2Document1 pageMorpot Interna 2IsnaNo ratings yet
- Clinical Management Multiple Drugs TBDocument10 pagesClinical Management Multiple Drugs TBIsnaNo ratings yet
- Art:10.1186/s13054 016 1252 2Document9 pagesArt:10.1186/s13054 016 1252 2IsnaNo ratings yet
- Childhood AsthmaDocument9 pagesChildhood Asthmanaufal12345No ratings yet
- Art:10.1186/s13063 017 1863 1 PDFDocument7 pagesArt:10.1186/s13063 017 1863 1 PDFIsnaNo ratings yet
- Recurent Pneumonia Among Jpanese AdultDocument9 pagesRecurent Pneumonia Among Jpanese Adultnaufal12345No ratings yet
- 2014 AF GuidelineDocument58 pages2014 AF GuidelineIsnaNo ratings yet
- Pediatric EM PDFDocument11 pagesPediatric EM PDFIsnaNo ratings yet
- Skin Graft & FlapsDocument17 pagesSkin Graft & FlapsRahul DeshmukhNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
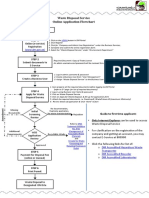
- Online Application FlowchartDocument2 pagesOnline Application FlowchartAnonymous u7Zq9FZkq100% (1)
- Extemporaneous CompoundingDocument4 pagesExtemporaneous Compoundingnita_ninotNo ratings yet
- Animal Testing in MedicineDocument9 pagesAnimal Testing in MedicineCamilla SatteNo ratings yet
- Chemical ContactDocument118 pagesChemical ContactkasvikrajNo ratings yet
- Pre-Filled Syringes 2014-2024 PDFDocument24 pagesPre-Filled Syringes 2014-2024 PDFVisiongainGlobal0% (1)
- Pharmaceutical Science 2014Document24 pagesPharmaceutical Science 2014lovehope100% (1)
- Bio Medicine - Atwood D.gainesDocument24 pagesBio Medicine - Atwood D.gainesden7770% (1)
- Case 6 Mylans Acquisition of MatrixDocument25 pagesCase 6 Mylans Acquisition of MatrixashmitNo ratings yet
- Essensial DrugDocument363 pagesEssensial Drugwilliam28asshole100% (1)
- DRL Case AnalysisDocument24 pagesDRL Case AnalysisPrabin PaudelNo ratings yet
- PGX TestingDocument51 pagesPGX TestingHashim KhanNo ratings yet
- Pharmaceutical Research and DevelopmentDocument4 pagesPharmaceutical Research and DevelopmentVarun BakshiNo ratings yet
- Cipla LTDDocument6 pagesCipla LTDSana AnjumNo ratings yet
- Nottingham Community Child Care Parent HandbookDocument8 pagesNottingham Community Child Care Parent Handbookapi-275291587No ratings yet
- Markans PharmaDocument19 pagesMarkans PharmaViju K GNo ratings yet
- Post OP InstructDocument2 pagesPost OP InstructNew Haven Oral SurgeryNo ratings yet
- GSKDocument4 pagesGSKMary Sugui0% (1)
- (Theory and Practice in Medical Anthropology and International Health, v. 3) Mark Nichter - Mimi Nichter-Anthropology and International Health - Asian Case Studies-Gordon and Breach (1996) PDFDocument486 pages(Theory and Practice in Medical Anthropology and International Health, v. 3) Mark Nichter - Mimi Nichter-Anthropology and International Health - Asian Case Studies-Gordon and Breach (1996) PDFjjason12345No ratings yet
- Pharmacy Service AgreementDocument164 pagesPharmacy Service AgreementChrissieNo ratings yet
- Strategic Management ProjectDocument84 pagesStrategic Management ProjectTalha Abdul Rauf57% (7)
- Ethics in Pharmaceutical Marketing PDFDocument2 pagesEthics in Pharmaceutical Marketing PDFKevinNo ratings yet
- Killer Copywriting Feb20 SDocument173 pagesKiller Copywriting Feb20 SNouveau Riche89% (9)
- Hospital Administration Role in Quality PatientcareDocument41 pagesHospital Administration Role in Quality PatientcareMuhammad Abeesh100% (2)
- Patients Rights and ResponsibilitiesDocument18 pagesPatients Rights and ResponsibilitiesmuthurajathiNo ratings yet
- New Microsoft Office Word DocumentDocument66 pagesNew Microsoft Office Word DocumentThanveer MaNo ratings yet
- Medicinal ChemistryDocument2 pagesMedicinal ChemistryKrisz KovácsNo ratings yet
- How To Kill CancerDocument88 pagesHow To Kill Cancerkalpesh deora100% (2)
- KlienDocument47 pagesKlientareq.sefatNo ratings yet
- Unfinished Agenda - Indian Molecule Going Global - Business Line PDFDocument2 pagesUnfinished Agenda - Indian Molecule Going Global - Business Line PDFhappinessalways38No ratings yet