You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Metabical Case StudyDocument2 pagesMetabical Case StudyLisa SNo ratings yet
- Standards of Perioperative Nursing by AORN 2016Document16 pagesStandards of Perioperative Nursing by AORN 2016Rudy Duterte100% (1)
- 50 Suspects 86 ChargesDocument3 pages50 Suspects 86 ChargesNewsWCYBDigitalNo ratings yet
- Capstone PharmDocument5 pagesCapstone Pharmmaria60% (5)
- Sophisticated Simple SentenceDocument1 pageSophisticated Simple SentenceRudy DuterteNo ratings yet
- Administering Vaginal InstillationsDocument6 pagesAdministering Vaginal InstillationsRudy DuterteNo ratings yet
- Compound Sentence: Coordinating Conjunction Conjunctive Adverb SemicolonDocument1 pageCompound Sentence: Coordinating Conjunction Conjunctive Adverb SemicolonRudy DuterteNo ratings yet
- Managing Fatigue Sue IrelandDocument30 pagesManaging Fatigue Sue IrelandRudy DuterteNo ratings yet
- Managing Fatigue Sue IrelandDocument30 pagesManaging Fatigue Sue IrelandRudy DuterteNo ratings yet
- Orientation of The Registered Nurses and Cetified Surgical Technologist To The Perioperative SettingDocument6 pagesOrientation of The Registered Nurses and Cetified Surgical Technologist To The Perioperative SettingRudy DuterteNo ratings yet
- AORN Electrosurgery GuidelinesDocument20 pagesAORN Electrosurgery GuidelinesRudy DuterteNo ratings yet
- Aorn Proposed Guidelines For Sterile TechniqueDocument104 pagesAorn Proposed Guidelines For Sterile TechniqueRudy DuterteNo ratings yet
- Implementing Aorn Recommended Practices For Environmental CleaningDocument13 pagesImplementing Aorn Recommended Practices For Environmental CleaningRudy DuterteNo ratings yet
- Aorn Position Statement On Perioperative Care of Patients With Do-Not-Resucitate or Allow-natural-Death OrdersDocument5 pagesAorn Position Statement On Perioperative Care of Patients With Do-Not-Resucitate or Allow-natural-Death OrdersRudy DuterteNo ratings yet
- Spasmolytic DrugsDocument3 pagesSpasmolytic DrugsVikash LamaNo ratings yet
- Summarised Clinchers Created For The Exam - Credits - Audi Maglalang-ReedDocument9 pagesSummarised Clinchers Created For The Exam - Credits - Audi Maglalang-ReedflashjetNo ratings yet
- Neonatal Drugs Section Fifth Edition2012 PDFDocument163 pagesNeonatal Drugs Section Fifth Edition2012 PDFAhmed MohammedNo ratings yet
- Development of Push-Pull Osmotic Pump Tablets For A SlightlyDocument4 pagesDevelopment of Push-Pull Osmotic Pump Tablets For A SlightlyphamuyenthuNo ratings yet
- Mucoadhesive System - PPT - Vijay BhaskarDocument60 pagesMucoadhesive System - PPT - Vijay Bhaskarboddarambabu100% (2)
- Principles of Drug AdministrationDocument4 pagesPrinciples of Drug Administrationlei ruminganNo ratings yet
- Family MedicineDocument156 pagesFamily MedicinedtriggNo ratings yet
- Sample Patient ContractDocument3 pagesSample Patient ContractImc AyurvedNo ratings yet
- Draft Report On InductionDocument72 pagesDraft Report On InductionSwati CherryNo ratings yet
- Diclegis Full Prescribing InformationDocument12 pagesDiclegis Full Prescribing Informationks2No ratings yet
- Dina-Farouk Q - A NotesDocument120 pagesDina-Farouk Q - A Notesraju niraulaNo ratings yet
- Table of Content PDFDocument5 pagesTable of Content PDFTech NestNo ratings yet
- DermatologyDocument1 pageDermatologyapi-251804148No ratings yet
- Sweating in Advanced Cancer (R. Twycross)Document11 pagesSweating in Advanced Cancer (R. Twycross)docbinNo ratings yet
- 021218drug Study CetirizineDocument2 pages021218drug Study Cetirizineliza sian100% (1)
- Psychiatric MedicationDocument22 pagesPsychiatric MedicationSofia Centro TaerNo ratings yet
- Signa ApotekDocument141 pagesSigna Apotekartapena1302No ratings yet
- Student Tox LectureDocument49 pagesStudent Tox Lecturelenin_villaltaNo ratings yet
- Morning ReportDocument31 pagesMorning Reports1882No ratings yet
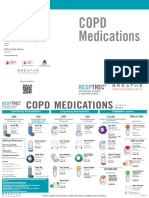
- Courses Offered:: Copd MedicationsDocument2 pagesCourses Offered:: Copd MedicationsDave BoyNo ratings yet
- Multiple IV Bolus AdministrationDocument21 pagesMultiple IV Bolus AdministrationIka NurzijahNo ratings yet
- Narcan InfographicDocument1 pageNarcan InfographicAnonymous C7bFTkrd5No ratings yet
- Types of Tablets and Their CharecteristicsDocument49 pagesTypes of Tablets and Their CharecteristicsRohit IrkalNo ratings yet
- Dosage - Chapter 10Document9 pagesDosage - Chapter 10kaukau4everNo ratings yet
- Chemotherapy: Al-Fahad J. Edding Franco Ben BelarminoDocument16 pagesChemotherapy: Al-Fahad J. Edding Franco Ben BelarminoSherina W. EddingNo ratings yet
- Standards For Medicines ManagementDocument112 pagesStandards For Medicines ManagementHélder AntunesNo ratings yet
- Spesialite ObatDocument15 pagesSpesialite ObatDovan Anfield GenkNo ratings yet