You might also like
- Postural reactions predict cerebral palsy riskDocument5 pagesPostural reactions predict cerebral palsy riskHéctor MartínezNo ratings yet
- Winters TF 1987 Gait Patterns in Spastic Hemiplegia in Children and Young AdultsDocument6 pagesWinters TF 1987 Gait Patterns in Spastic Hemiplegia in Children and Young AdultsEileen Torres CerdaNo ratings yet
- Five New Cases and Review of Nine Previously Published CasesDocument8 pagesFive New Cases and Review of Nine Previously Published CasesBogdan SoptereanNo ratings yet
- Neurological Development From Birth To Six YearsDocument143 pagesNeurological Development From Birth To Six YearsWaleska SakibNo ratings yet
- Vestibular Evoked Myogenic Potentials in ChildrenDocument5 pagesVestibular Evoked Myogenic Potentials in ChildrenCanto XChileNo ratings yet
- DesarrolloDocument143 pagesDesarrolloPablo Antonio AntonioNo ratings yet
- (31 36) V9N5PTDocument6 pages(31 36) V9N5PTASD2019No ratings yet
- Piis0002713809601151 PDFDocument6 pagesPiis0002713809601151 PDFLuwinda SariNo ratings yet
- VentrikulomegaliDocument6 pagesVentrikulomegaliAida NurwidyaNo ratings yet
- SCIWORA-Spinal Cord Injury Without Radiological Abnormality: Veena Kalra, Sheffali Gulati, Mahesh Kamate and Ajay GargDocument3 pagesSCIWORA-Spinal Cord Injury Without Radiological Abnormality: Veena Kalra, Sheffali Gulati, Mahesh Kamate and Ajay GargnsatriotomoNo ratings yet
- P ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Document6 pagesP ('t':3) Var B Location Settimeout (Function (If (Typeof Window - Iframe 'Undefined') (B.href B.href ) ), 15000)Riri KumalaNo ratings yet
- Trunk Recruitment During Spoon Use in Tetraparetic Cerebral PalsyDocument10 pagesTrunk Recruitment During Spoon Use in Tetraparetic Cerebral Palsykashif salmanNo ratings yet
- Materials and Methods PatientsDocument1 pageMaterials and Methods PatientsZainuddin Surkan HNo ratings yet
- Prevalence of Vertigo in Different Age Groups and Common Butterfly Patterns in Electronystagmography in Central India: A Retrospective StudyDocument8 pagesPrevalence of Vertigo in Different Age Groups and Common Butterfly Patterns in Electronystagmography in Central India: A Retrospective StudyIOSRjournalNo ratings yet
- Estriado Durston - Biol.psychDocument8 pagesEstriado Durston - Biol.psychManuel PasteneNo ratings yet
- Ukuran Hepar Lien Pada AnakDocument6 pagesUkuran Hepar Lien Pada Anakivan ekoNo ratings yet
- Ben SonDocument5 pagesBen SonDian NovitasariNo ratings yet
- Jauregui 2017Document9 pagesJauregui 2017Bison_sonNo ratings yet
- Post Viral Encephalitis Sequelae and Their RehabilitationDocument2 pagesPost Viral Encephalitis Sequelae and Their RehabilitationRizka KusumaningsihNo ratings yet
- US Hip TechniqueDocument8 pagesUS Hip TechniqueAdam JonesNo ratings yet
- Arch Dis Child Fetal Neonatal Ed-2005 5876Document6 pagesArch Dis Child Fetal Neonatal Ed-2005 5876Dian NovitasariNo ratings yet
- Epilepsy and Electroencephalogram Evolution in YWHAG Gene MutationDocument8 pagesEpilepsy and Electroencephalogram Evolution in YWHAG Gene MutationGiselle Costa Daniel HonoratoNo ratings yet
- PDD Case with Chromosome 1-4 TranslocationDocument14 pagesPDD Case with Chromosome 1-4 TranslocationAgustia Pratiwi AhmadNo ratings yet
- The Evolution of Primitive Reflexes in Extremely Premature InfantsDocument6 pagesThe Evolution of Primitive Reflexes in Extremely Premature InfantsPriydarshni KohliNo ratings yet
- Long-Term Steroid Therapy for Asthma PatientsDocument5 pagesLong-Term Steroid Therapy for Asthma PatientsMinerva StanciuNo ratings yet
- Brief Report: Does Eye Contact Induce Contagious Yawning in Children With Autism Spectrum Disorder?Document6 pagesBrief Report: Does Eye Contact Induce Contagious Yawning in Children With Autism Spectrum Disorder?Pakde Putu HadiNo ratings yet
- Large Arachnoid Cyst: T. Mondal K. Jagdish Kumar R. Anand N.K. Dubey D. SharmaDocument3 pagesLarge Arachnoid Cyst: T. Mondal K. Jagdish Kumar R. Anand N.K. Dubey D. SharmaJaya PrabhaNo ratings yet
- Epilepsy in Children With Shunted HydrocephalusDocument16 pagesEpilepsy in Children With Shunted HydrocephalusPauleen Trisha SamparaniNo ratings yet
- MR Imaging Characteristics of Tuberculous Spondylitis Vertebral OsteomyelitisDocument7 pagesMR Imaging Characteristics of Tuberculous Spondylitis Vertebral OsteomyelitislewienNo ratings yet
- Journal Homepage: - : Manuscript HistoryDocument6 pagesJournal Homepage: - : Manuscript HistoryIJAR JOURNALNo ratings yet
- Periodic Breathing in Patients With NALCN Mutations: Clinical ReportDocument4 pagesPeriodic Breathing in Patients With NALCN Mutations: Clinical ReportIvan VeriswanNo ratings yet
- New Therapies For Rett SyndromeDocument7 pagesNew Therapies For Rett SyndromeAamir Jalal Al-MosawiNo ratings yet
- US Features Help Differentiate Types of Intussusception in ChildrenDocument6 pagesUS Features Help Differentiate Types of Intussusception in ChildrenTrii MNo ratings yet
- Brain Volume and Shape in Infants With Deformational PlagiocephalyDocument8 pagesBrain Volume and Shape in Infants With Deformational PlagiocephalychiaraNo ratings yet
- Bruni-2004-Sleep Disturbances in As A Questionnaire StudyDocument8 pagesBruni-2004-Sleep Disturbances in As A Questionnaire Studybappi11No ratings yet
- Screening 2Document6 pagesScreening 2Yariel AraujoNo ratings yet
- Genu Valgum and Flat Feet in Children With Healthy.15Document7 pagesGenu Valgum and Flat Feet in Children With Healthy.15saarita lozano piedraNo ratings yet
- Profil Epilepsi Anak Dan Keberhasilan Pengobatannya Di RSUD Dr. Soetomo Tahun 2013Document6 pagesProfil Epilepsi Anak Dan Keberhasilan Pengobatannya Di RSUD Dr. Soetomo Tahun 2013Pramusetya SuryandaruNo ratings yet
- NIH Public Access: Cerebral Hemispherectomy: Sensory Scores Before and After Intensive Mobility TrainingDocument11 pagesNIH Public Access: Cerebral Hemispherectomy: Sensory Scores Before and After Intensive Mobility TrainingBimantoro SaputroNo ratings yet
- Changing Pattern of CP in The Southwest Region of FinlandDocument7 pagesChanging Pattern of CP in The Southwest Region of FinlandЯковлев АлександрNo ratings yet
- Sindrom PatauDocument12 pagesSindrom PatauIoana PaulaNo ratings yet
- Develop Med Child Neuro - 2007 - KR Geloh Mann - Bilateral Lesions of Thalamus and Basal Ganglia Origin and OutcomeDocument8 pagesDevelop Med Child Neuro - 2007 - KR Geloh Mann - Bilateral Lesions of Thalamus and Basal Ganglia Origin and OutcomeValentina RusuNo ratings yet
- Outcome in Childhood Guillain-Barré SyndromeDocument5 pagesOutcome in Childhood Guillain-Barré SyndromechristianFPTNo ratings yet
- Abduction Treatment in Stable Hip Dysplasia Does Not Alter The Acetabular Growth: Results of A Randomized Clinical TrialDocument7 pagesAbduction Treatment in Stable Hip Dysplasia Does Not Alter The Acetabular Growth: Results of A Randomized Clinical TrialRoyman MejiaNo ratings yet
- Pediatric Orbital Rhabdomyosarcoma OutcomesDocument7 pagesPediatric Orbital Rhabdomyosarcoma OutcomesNurul RiskiNo ratings yet
- The Developing Anterior Skull Base: CT Appearance From Birth To 2 Years of AgeDocument8 pagesThe Developing Anterior Skull Base: CT Appearance From Birth To 2 Years of AgeKumaran Bagavathi RagavanNo ratings yet
- Pediatrie DimensiuniDocument6 pagesPediatrie DimensiuniDanaAmaranducaiNo ratings yet
- Jurnal Internasional 1Document5 pagesJurnal Internasional 1As karNo ratings yet
- Proceedings of The 2014 Spring Meeting of The Society of British 2014Document40 pagesProceedings of The 2014 Spring Meeting of The Society of British 2014rabiatul adawiyahNo ratings yet
- Precht L 1997Document3 pagesPrecht L 1997Javiera Rodriguez QuezadaNo ratings yet
- Magnetic Resonance DetectionDocument5 pagesMagnetic Resonance DetectionEoin O'MalleyNo ratings yet
- 2006 Fetal and Infant EDITORIAL Hart - Developmental - Medicine - & - Child - NeurologyDocument1 page2006 Fetal and Infant EDITORIAL Hart - Developmental - Medicine - & - Child - NeurologyDamara GardelNo ratings yet
- Prevention of DislocationDocument7 pagesPrevention of DislocationRolando Hdez RuizNo ratings yet
- RX Utiles DCDDocument4 pagesRX Utiles DCDAlicia BallesterosNo ratings yet
- Research Article: Correlation Between TMD and Cervical Spine Pain and Mobility: Is The Whole Body Balance TMJ Related?Document8 pagesResearch Article: Correlation Between TMD and Cervical Spine Pain and Mobility: Is The Whole Body Balance TMJ Related?gloriagaskNo ratings yet
- CP Spastic, Diskinetik, AtaxicDocument4 pagesCP Spastic, Diskinetik, AtaxicNura Eky VNo ratings yet
- Tsukahara 1997Document5 pagesTsukahara 1997Narjes Sharif AskariNo ratings yet
- Asian Nursing Research: Nejla Canbulat, PHD, Sevil - Inal, PHD, Hacer Sönmezer, MSCDocument6 pagesAsian Nursing Research: Nejla Canbulat, PHD, Sevil - Inal, PHD, Hacer Sönmezer, MSCMarnia SulfianaNo ratings yet
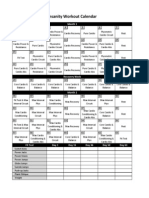
- Cronograma InsanityDocument1 pageCronograma InsanityCatherine EcheverryNo ratings yet
- Antagonistas de Los Receptores NMDA Dolor CrónicoDocument13 pagesAntagonistas de Los Receptores NMDA Dolor CrónicoMario Viazcan CarbajalNo ratings yet
- Analysis of The Pattern of Suprahyoid Muscle Activity During Pharyngeal Swallowing of Foods by Healthy Young SubjectsDocument7 pagesAnalysis of The Pattern of Suprahyoid Muscle Activity During Pharyngeal Swallowing of Foods by Healthy Young SubjectsFabian Esteban SubiabreNo ratings yet
- Early Intervention in The NeurodevelopmentDocument6 pagesEarly Intervention in The NeurodevelopmentFabian Esteban Subiabre100% (1)
- Roberto Merletti, Multi Channel Surface EMG For The Non Invasive Assessment of The Anal Sphincter Muscle 2004 Digestion PortoDocument26 pagesRoberto Merletti, Multi Channel Surface EMG For The Non Invasive Assessment of The Anal Sphincter Muscle 2004 Digestion PortoFabian Esteban SubiabreNo ratings yet
- Analysis of The Pattern of Suprahyoid Muscle Activity During Pharyngeal Swallowing of Foods by Healthy Young SubjectsDocument7 pagesAnalysis of The Pattern of Suprahyoid Muscle Activity During Pharyngeal Swallowing of Foods by Healthy Young SubjectsFabian Esteban SubiabreNo ratings yet
- Deluca Surface Electromyography Detection&RecordingDocument10 pagesDeluca Surface Electromyography Detection&RecordingJuan Rodriguez IIINo ratings yet
- Ooool - Biomecanica Craneo - Cervical y ATMDocument30 pagesOoool - Biomecanica Craneo - Cervical y ATMFabian Esteban SubiabreNo ratings yet
- Ventlacionmecanica ASMADocument10 pagesVentlacionmecanica ASMAFabian Esteban SubiabreNo ratings yet
- NAVA HypoventilationDocument3 pagesNAVA HypoventilationFabian Esteban SubiabreNo ratings yet
- Prevention of Endotracheal Suctioning-Induced Alveolar Derecruitment in Acute Lung InjuryDocument54 pagesPrevention of Endotracheal Suctioning-Induced Alveolar Derecruitment in Acute Lung InjuryFabian Esteban SubiabreNo ratings yet
- Update en EpocDocument9 pagesUpdate en EpocFabian Esteban SubiabreNo ratings yet
- Patient Ventilator Asynchronies May TheDocument8 pagesPatient Ventilator Asynchronies May TheFabian Esteban SubiabreNo ratings yet
- Depuracion de Mucus en Las Vias AereasDocument7 pagesDepuracion de Mucus en Las Vias AereasFabian Esteban SubiabreNo ratings yet
- Physiology of Mechanical VentilationDocument18 pagesPhysiology of Mechanical VentilationLiliana Andrea Hurtado MeraNo ratings yet
- A Chart of Failure Risk For NoninvasiveDocument8 pagesA Chart of Failure Risk For NoninvasiveFabian Esteban SubiabreNo ratings yet
- Citacion Vancouver PapersDocument1 pageCitacion Vancouver PapersFabian Esteban SubiabreNo ratings yet
- 116 093 Agustiag Oxygen Therapy During Exacerbations CopdDocument6 pages116 093 Agustiag Oxygen Therapy During Exacerbations CopdFabian Esteban SubiabreNo ratings yet
- The Effects of Orthostatism in Adult Intensive Care Unit PatientsDocument8 pagesThe Effects of Orthostatism in Adult Intensive Care Unit PatientsFabian Esteban SubiabreNo ratings yet
- Extubation Failure Magnitude of The ProblemDocument8 pagesExtubation Failure Magnitude of The ProblemFabian Esteban SubiabreNo ratings yet
- Endotracheal Suctioning of Mechanically Ventilated Patients With Artificial Airways (June 2010)Document7 pagesEndotracheal Suctioning of Mechanically Ventilated Patients With Artificial Airways (June 2010)DCaeiroNo ratings yet
- 2015 Early Mobilization in The Critical Care Unit, A Review of Adult and Pediatric LiteratureDocument9 pages2015 Early Mobilization in The Critical Care Unit, A Review of Adult and Pediatric LiteratureFabian Esteban SubiabreNo ratings yet
- Fem 3202-1 IntroductionDocument29 pagesFem 3202-1 IntroductionRon ChongNo ratings yet
- Quartz Textures in Epithermal VeinsDocument16 pagesQuartz Textures in Epithermal VeinsAlvaro MadridNo ratings yet
- Tools and EquipmentDocument30 pagesTools and EquipmentEhm Jhay78% (9)
- Postnatal Care, Complaints & AbnormalitiesDocument38 pagesPostnatal Care, Complaints & AbnormalitiesBernice GyapongNo ratings yet
- PKL Geri RevDocument3 pagesPKL Geri RevKurniati NiaNo ratings yet
- TN EpasssDocument2 pagesTN EpasssStephenrajNo ratings yet
- Paper TropicsDocument8 pagesPaper Tropicsdarobin21No ratings yet
- NCPDocument18 pagesNCPChristian Karl B. LlanesNo ratings yet
- Recent Developments in Carbapenems: ReviewDocument16 pagesRecent Developments in Carbapenems: ReviewFrancielleNo ratings yet
- Marital Rape in IndiaDocument8 pagesMarital Rape in IndiaSHUBHANK SUMANNo ratings yet
- Mms For Household Uses-S.pardee-1Document7 pagesMms For Household Uses-S.pardee-1Manny JorgeNo ratings yet
- Understand TSGLI BenefitsDocument2 pagesUnderstand TSGLI BenefitsJoseph LawerenceNo ratings yet
- Ate-U2 - Steam Boilers - PPT - Session 3Document13 pagesAte-U2 - Steam Boilers - PPT - Session 3MANJU R BNo ratings yet
- Stakeholders in The Iep Process JDocument9 pagesStakeholders in The Iep Process Japi-546526887No ratings yet
- 6d Class 10Document10 pages6d Class 10Euna DawkinsNo ratings yet
- READING MODULE 4 - CompressedDocument13 pagesREADING MODULE 4 - CompressedPaolo IcangNo ratings yet
- Catalogo - Itens 10 e 34Document15 pagesCatalogo - Itens 10 e 34Anderson Silva CarvalhoNo ratings yet
- Effects of Climate Change and Global WarmingDocument14 pagesEffects of Climate Change and Global WarmingSwetal SosaNo ratings yet
- Non Ferrous AlloysDocument45 pagesNon Ferrous AlloysDeepak NegiNo ratings yet
- CAP - 5 - 54. Billions and Billions of Demons - by Richard C. Lewontin - The New York Review of BooksDocument11 pagesCAP - 5 - 54. Billions and Billions of Demons - by Richard C. Lewontin - The New York Review of BooksRaimundo Filho100% (1)
- Pastillas DelightDocument12 pagesPastillas DelightBryan DutchaNo ratings yet
- We Get Results!: Spring FlingDocument35 pagesWe Get Results!: Spring FlingThe WorldNo ratings yet
- Menu Selector - Hyatt Regency LucknowDocument11 pagesMenu Selector - Hyatt Regency LucknowShoubhik SinhaNo ratings yet
- Phychem Expt. 1Document8 pagesPhychem Expt. 1Bren Julius PabloNo ratings yet
- CAUTI Surveillance FormDocument2 pagesCAUTI Surveillance FormJiansong ChangNo ratings yet
- PositionsDocument4 pagesPositionsMixsz LlhAdyNo ratings yet
- Jurnal ResinDocument8 pagesJurnal ResinRizky Febrian SatrianiNo ratings yet
- Lecture 4 Part 1 PDFDocument11 pagesLecture 4 Part 1 PDFBashar AntriNo ratings yet
- Fault Location of Overhead Transmission Line With Noncontact Magnetic Field MeasurementDocument10 pagesFault Location of Overhead Transmission Line With Noncontact Magnetic Field MeasurementJkNo ratings yet
- On Prem Vs CloudDocument10 pagesOn Prem Vs CloudJeev AnandNo ratings yet