You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- G-Cem Capsule: Prior To Use, Carefully Read The Instructions For UseDocument1 pageG-Cem Capsule: Prior To Use, Carefully Read The Instructions For UseAndrea LawNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Tetric LineDocument10 pagesTetric LineAndrea LawNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Selection of Articulator For General Dental PractiDocument6 pagesSelection of Articulator For General Dental PractiAayushi VaidyaNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Empress Direct - Special - Mahn - en - 678773 - PRINT PDFDocument48 pagesEmpress Direct - Special - Mahn - en - 678773 - PRINT PDFKhalil SalahNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Uses of Dental Wax in Clinics and LaboratoriesDocument2 pagesUses of Dental Wax in Clinics and LaboratoriesAndrea LawNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- InTech-Bone Quality Assessment For Dental ImplantsDocument17 pagesInTech-Bone Quality Assessment For Dental ImplantsMohamed Abd El-Fattah GalalNo ratings yet
- Dental WaxDocument14 pagesDental WaxAndrea LawNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- DENTAL MATERIALS Biocompat RedoDocument17 pagesDENTAL MATERIALS Biocompat RedoAndrea LawNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Daftar PustakaDocument5 pagesDaftar PustakaAndrea LawNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Clinical Significance of Accessory Foramina in AduDocument6 pagesClinical Significance of Accessory Foramina in AduAndrea LawNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- 016 Andrea - Smile DesignDocument3 pages016 Andrea - Smile DesignAndrea LawNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Analytical Vs Descriptive ResearchDocument2 pagesAnalytical Vs Descriptive ResearchAndrea LawNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
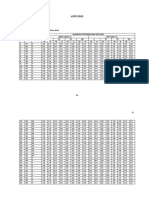
- Appendix: Appendix 1 Master Table Alveolar Bone Resorption DataDocument12 pagesAppendix: Appendix 1 Master Table Alveolar Bone Resorption DataAndrea LawNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- 5 CementoenamelDocument8 pages5 CementoenamelAndrea LawNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Bone Resorption Increases with Age and Differs between GendersDocument1 pageBone Resorption Increases with Age and Differs between GendersAndrea LawNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 016-Malignant Tumours of The Oral CavityDocument11 pages016-Malignant Tumours of The Oral CavityAndrea LawNo ratings yet
- 016 ImpactionDocument9 pages016 ImpactionAndrea LawNo ratings yet
- PedoDocument12 pagesPedoAndrea LawNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- 016 Andrea - Smile DesignDocument3 pages016 Andrea - Smile DesignAndrea LawNo ratings yet
- Topic 3 Dentoalveolar FractureDocument56 pagesTopic 3 Dentoalveolar FractureAndrea LawNo ratings yet
- AdenddumsDocument16 pagesAdenddumsAndrea LawNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Index of RefractionDocument3 pagesIndex of RefractionAndrea LawNo ratings yet
- General Technique of Third Molar Removal, Bouloux G.F. 2007Document21 pagesGeneral Technique of Third Molar Removal, Bouloux G.F. 2007Felipe Ronceros100% (1)
- 016-017 Diagnosis of Case 5Document3 pages016-017 Diagnosis of Case 5Andrea LawNo ratings yet
- DSP 9 Case 5 Tooth FractureDocument39 pagesDSP 9 Case 5 Tooth FractureAndrea LawNo ratings yet
- Sex Steroid and The BoneDocument29 pagesSex Steroid and The BoneAndrea LawNo ratings yet
- 016 Andrea - Smile DesignDocument3 pages016 Andrea - Smile DesignAndrea LawNo ratings yet
- Preprosthetic SurgeryDocument4 pagesPreprosthetic SurgeryDentist HereNo ratings yet
- Example Adult Maxillary Anterior Occlusal Radiograph.: SourceDocument2 pagesExample Adult Maxillary Anterior Occlusal Radiograph.: SourceAndrea LawNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Environmental Modeling and Health Risk AnalysisESTEDocument478 pagesEnvironmental Modeling and Health Risk AnalysisESTESantiago Cardona GalloNo ratings yet
- Frequently Asked Questions On The RH BillDocument15 pagesFrequently Asked Questions On The RH BillMulat Pinoy-Kabataan News Network100% (2)
- Jurnal IMD 2Document11 pagesJurnal IMD 2weniNo ratings yet
- 4 - Chapter - Respiratory SystemDocument25 pages4 - Chapter - Respiratory SystemleonNo ratings yet
- Importance of Community Health NursingDocument1 pageImportance of Community Health NursingJunghoon YangParkNo ratings yet
- Route of Drug AdministrationDocument4 pagesRoute of Drug AdministrationMr. PREMNATH D. 930No ratings yet
- SHS Applied - Inquiries, Investigations and Immersions CG - Spideylab - Com - 2017Document4 pagesSHS Applied - Inquiries, Investigations and Immersions CG - Spideylab - Com - 2017Lexis Anne BernabeNo ratings yet
- WHO IVB 12.10 EngDocument36 pagesWHO IVB 12.10 EngJjNo ratings yet
- An Introduction To Spanish For Health Care Workers Communication and Culture, 3e (2010)Document398 pagesAn Introduction To Spanish For Health Care Workers Communication and Culture, 3e (2010)johngaltjeep100% (5)
- Junk Food's Harmful Effects and Healthy SolutionsDocument18 pagesJunk Food's Harmful Effects and Healthy SolutionsMarcela CoroleaNo ratings yet
- Test Bank For Delmars Administrative Medical Assisting 5th EditionDocument7 pagesTest Bank For Delmars Administrative Medical Assisting 5th Editionloriandersonbzrqxwnfym100% (31)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Data Obs Covid Januari-Juli 2021Document15 pagesData Obs Covid Januari-Juli 2021primaindra27No ratings yet
- Hospital ExamplesDocument10 pagesHospital ExamplesArmand Kyle AbadNo ratings yet
- Stress Reduction ActivityDocument4 pagesStress Reduction ActivityBramwel Muse (Gazgan bram)No ratings yet
- CASE STUDY MeningitisDocument19 pagesCASE STUDY Meningitissonal aranha100% (3)
- Diagnose Poultry Diseases AccuratelyDocument24 pagesDiagnose Poultry Diseases AccuratelyAbdul Hai ChowdhuryNo ratings yet
- Project Report On Stress ManagementDocument73 pagesProject Report On Stress ManagementPriya KuttyNo ratings yet
- Moore 2013Document11 pagesMoore 2013JulioRoblesZanelliNo ratings yet
- Hazard Analysis and CCP DeterminationDocument2 pagesHazard Analysis and CCP DeterminationGaganpreet Kaur SainiNo ratings yet
- Nursing Care Plan Rheumatoid ArthritisDocument4 pagesNursing Care Plan Rheumatoid ArthritisLighto RyusakiNo ratings yet
- Rhetorical Analysis Essay-4Document5 pagesRhetorical Analysis Essay-4api-545696216No ratings yet
- BFCI Annexes 1Document60 pagesBFCI Annexes 1BrianBeauttahNo ratings yet
- Lessons Learnt During Malaysia's MCODocument2 pagesLessons Learnt During Malaysia's MCOYEW SIAU JING MoeNo ratings yet
- Fish OilDocument44 pagesFish OilRamchandra Keny50% (2)
- JSA-070 Desert Road TripDocument4 pagesJSA-070 Desert Road TripMoaatazz NouisriNo ratings yet
- Effect of Different Types of Anesthesia On.23 PDFDocument5 pagesEffect of Different Types of Anesthesia On.23 PDFHelsie DahokloryNo ratings yet
- IJM Safety Conference Paper Summarizes NADOPOD 2004 Reporting RegulationsDocument1 pageIJM Safety Conference Paper Summarizes NADOPOD 2004 Reporting RegulationsKay AayNo ratings yet
- HC Fruits VeggiesDocument4 pagesHC Fruits VeggiesshallovesuNo ratings yet
- Nature's Role in Reducing Mental FatigueDocument9 pagesNature's Role in Reducing Mental FatigueCrăciun RalucaNo ratings yet
- Benefitfocus For LifeDocument7 pagesBenefitfocus For LifeLacey WoolstonNo ratings yet