You might also like
- Illustrations Of Special Effective Acupoints for common DiseasesFrom EverandIllustrations Of Special Effective Acupoints for common DiseasesNo ratings yet
- The Treatment of Ovarian Hyperstimulation Syndrome (OHSS) With Acupuncture in Women Undergoing Assisted Reproductive Techniques (ART)Document9 pagesThe Treatment of Ovarian Hyperstimulation Syndrome (OHSS) With Acupuncture in Women Undergoing Assisted Reproductive Techniques (ART)InfohoggNo ratings yet
- Axis of Efficacy Part-2Document9 pagesAxis of Efficacy Part-2Raoul GroulsNo ratings yet
- A Historical Review of Acupuncture To The Achilles TendonDocument10 pagesA Historical Review of Acupuncture To The Achilles TendonCrystal SalasNo ratings yet
- The Treatment of Psycho-Emotional Disturbance by Acupuncture With Particular Reference To The Du MaiDocument5 pagesThe Treatment of Psycho-Emotional Disturbance by Acupuncture With Particular Reference To The Du MaiPutu Abhihita SabdaNo ratings yet
- Acupoint Stimulation Effective for AcneDocument22 pagesAcupoint Stimulation Effective for AcneCristian SauraNo ratings yet
- Alchemical Facial Acupuncture Protocols, Part 3: by Mary Elizabeth Wakefield, Lac, Dipl. Ac., MS, MMDocument3 pagesAlchemical Facial Acupuncture Protocols, Part 3: by Mary Elizabeth Wakefield, Lac, Dipl. Ac., MS, MMHaryono zhuNo ratings yet
- The Acumoxa Treatment of Shoulder Impingement SyndromeDocument8 pagesThe Acumoxa Treatment of Shoulder Impingement SyndromeAngela PagliusoNo ratings yet
- Cancer GERA 2014Document238 pagesCancer GERA 2014zayarmyint_u100% (1)
- 361 Standard and 48 Extra (1001 - 1048) Acupuncture PointsDocument12 pages361 Standard and 48 Extra (1001 - 1048) Acupuncture PointsKesavadev100% (1)
- Diabetes MellitusDocument8 pagesDiabetes Mellitusab21423No ratings yet
- A Comprehesive TCM Approach To Diagnosis - CancerDocument8 pagesA Comprehesive TCM Approach To Diagnosis - CancerElizabeth Durkee Neil100% (1)
- Acupuncture For The Treatment of Chronic Painful Peripheral Diabetic Neuropathy: A Long-Term StudyDocument7 pagesAcupuncture For The Treatment of Chronic Painful Peripheral Diabetic Neuropathy: A Long-Term StudyFernanda GiulianoNo ratings yet
- Academia and Clinic: Acupuncture: Theory, Efficacy, and PracticeDocument10 pagesAcademia and Clinic: Acupuncture: Theory, Efficacy, and Practicedelaney771No ratings yet
- New Approach to Treating Female Infertility Integrates Chinese and Western MedicineDocument23 pagesNew Approach to Treating Female Infertility Integrates Chinese and Western Medicinean ssiNo ratings yet
- 王居易 The Clinical Significance of Palpable Channel Changes PDFDocument7 pages王居易 The Clinical Significance of Palpable Channel Changes PDFJose Gregorio ParraNo ratings yet
- Traditional Chinese Medicine Approach to DiabetesDocument6 pagesTraditional Chinese Medicine Approach to DiabetesFernanda GiulianoNo ratings yet
- TCM Acupuncture and Acupressure Effects on LaborDocument17 pagesTCM Acupuncture and Acupressure Effects on Laboramilyapradita100% (1)
- Professor Wang Juyi Interview: Acupuncture Achievements & Case StudiesDocument7 pagesProfessor Wang Juyi Interview: Acupuncture Achievements & Case StudiesYagtaliNo ratings yet
- Article Bahuang PointsDocument3 pagesArticle Bahuang PointsmudrahoraNo ratings yet
- Cosmetic Acu Yang - Yin4Document5 pagesCosmetic Acu Yang - Yin4janachidambaram100% (1)
- 06 Michelle GellisDocument7 pages06 Michelle Gellistigerstyle1No ratings yet
- Zhen Jiujia Yi JingDocument6 pagesZhen Jiujia Yi Jingsuperser123465No ratings yet
- A Christian Perspective of Acupuncture: A Research Paper Submitted To DR Keith WarringtonDocument33 pagesA Christian Perspective of Acupuncture: A Research Paper Submitted To DR Keith WarringtonEric TNo ratings yet
- Acupuncture Bell's Palsy RecoveryDocument7 pagesAcupuncture Bell's Palsy RecoveryJk SalvadorNo ratings yet
- The Spark in The MachineDocument53 pagesThe Spark in The MachineElanghovan Arumugam100% (1)
- Chong Mai (Parte 2)Document16 pagesChong Mai (Parte 2)Alexandre HenriquesNo ratings yet
- Emotions FruehaufDocument15 pagesEmotions FruehaufRomi BrenerNo ratings yet
- Understanding Jing Fang Formula Patterns Through Case StudiesDocument3 pagesUnderstanding Jing Fang Formula Patterns Through Case StudiesMatthieu DecalfNo ratings yet
- School of Febrile Diseases History Development DiagnosisDocument9 pagesSchool of Febrile Diseases History Development DiagnosisJaffer Aftab0% (1)
- Adv Acu Tech 1 - Class 1 - Jiao's Scalp AcupunctureDocument4 pagesAdv Acu Tech 1 - Class 1 - Jiao's Scalp Acupuncturesuperser123465No ratings yet
- ASA08 S6 MazinAlKhafaji PRESDocument22 pagesASA08 S6 MazinAlKhafaji PRESYagtaliNo ratings yet
- 55 10 PsoriasisDocument5 pages55 10 PsoriasisGabriel NavarroNo ratings yet
- Tefillin - An Ancient Acupuncture Point PrescriptionDocument4 pagesTefillin - An Ancient Acupuncture Point Prescriptionludofar100% (2)
- EM2 Webinar - DR - SteinerDocument131 pagesEM2 Webinar - DR - SteinerLukasNo ratings yet
- The Alchemy of Facial RenewalDocument4 pagesThe Alchemy of Facial RenewalHaryono zhuNo ratings yet
- Constipation/ - Bian Bi: ConceptionDocument3 pagesConstipation/ - Bian Bi: Conceptionnaeem_k7No ratings yet
- Diaphragmatic Reactivity and Stress ReactionsDocument10 pagesDiaphragmatic Reactivity and Stress Reactionsmamun31No ratings yet
- Wei SyndromeDocument8 pagesWei SyndromeezraallenNo ratings yet
- Chinese Fire CuppingDocument6 pagesChinese Fire Cuppingmd_corona62No ratings yet
- Lesson: Dr. Leon Hammer, M.DDocument12 pagesLesson: Dr. Leon Hammer, M.DRocío JMNo ratings yet
- Artemisia Vulgaris and the Art of MoxibustionDocument20 pagesArtemisia Vulgaris and the Art of MoxibustionG.No ratings yet
- Mother Child Points Theory and ApplicationsDocument3 pagesMother Child Points Theory and ApplicationsChetna Kanchan BhagatNo ratings yet
- Extra PointsDocument5 pagesExtra Pointsdelaney771No ratings yet
- Acupuncture For Disorders of ConsciousneswsDocument27 pagesAcupuncture For Disorders of ConsciousneswsGabriel Navarro100% (1)
- McDonald John - Chinese Versus French Perspectives On The Channel SystemDocument17 pagesMcDonald John - Chinese Versus French Perspectives On The Channel SystemAssaf FeldmanNo ratings yet
- The Ling Shu PrécisDocument9 pagesThe Ling Shu PrécisTim SchlankNo ratings yet
- A Revised Neuromyofascial Understanding For The Neck Head and Facial Channel Sinews Based On The Ling ShuDocument17 pagesA Revised Neuromyofascial Understanding For The Neck Head and Facial Channel Sinews Based On The Ling ShuAnonNo ratings yet
- PDF Post Stroke Scalp Acupuncture DLDocument64 pagesPDF Post Stroke Scalp Acupuncture DLyohan100% (2)
- The Neglected Art of Channel Palpation Part2Document6 pagesThe Neglected Art of Channel Palpation Part2gdupres66No ratings yet
- Shonishin - AcupDocument2 pagesShonishin - AcupKoa Carlos CastroNo ratings yet
- Acu Nou Si InteresantDocument276 pagesAcu Nou Si InteresantdoringramaNo ratings yet
- Acupuncture in Reproductive MedicineDocument13 pagesAcupuncture in Reproductive MedicineyohanNo ratings yet
- Managing Pain: And Other Medically Proven Uses of AcupunctureFrom EverandManaging Pain: And Other Medically Proven Uses of AcupunctureNo ratings yet
- The Acupuncture Prescription:: A Holistic Approach to HealthFrom EverandThe Acupuncture Prescription:: A Holistic Approach to HealthNo ratings yet
- Epilepsia - 2022 - Zuberi - ILAE Classification and Definition of Epilepsy Syndromes With Onset in Neonates and InfantsDocument49 pagesEpilepsia - 2022 - Zuberi - ILAE Classification and Definition of Epilepsy Syndromes With Onset in Neonates and InfantsAndres Rojas JerezNo ratings yet
- International League Against Epilepsy Classification and Definition of Epilepsy Syndromes With Onset in Childhood Position Paper by The ILAE Task Force On Nosology and DefinitionsDocument45 pagesInternational League Against Epilepsy Classification and Definition of Epilepsy Syndromes With Onset in Childhood Position Paper by The ILAE Task Force On Nosology and DefinitionsEduardo Rios DuboisNo ratings yet
- ACNS Training Module 2022-01-01 Part2 FINALDocument82 pagesACNS Training Module 2022-01-01 Part2 FINALAndres Rojas JerezNo ratings yet
- J Jvca 2015 03 020Document6 pagesJ Jvca 2015 03 020Andres Rojas JerezNo ratings yet
- J Clinph 2005 04 020Document11 pagesJ Clinph 2005 04 020Andres Rojas JerezNo ratings yet
- ACNS Training Module 2022-01-01 Part1 FINALDocument41 pagesACNS Training Module 2022-01-01 Part1 FINALAndres Rojas JerezNo ratings yet
- ACNS Training Module 2022-01-01 Combined FINALDocument153 pagesACNS Training Module 2022-01-01 Combined FINALAndres Rojas JerezNo ratings yet
- Ene 12372Document7 pagesEne 12372Andres Rojas JerezNo ratings yet
- Electroencephalography (EEG) in The Diagnosis of Seizures and Epilepsy - UpToDateDocument41 pagesElectroencephalography (EEG) in The Diagnosis of Seizures and Epilepsy - UpToDateAndres Rojas JerezNo ratings yet
- J Clinph 2013 03 031Document7 pagesJ Clinph 2013 03 031Andres Rojas JerezNo ratings yet
- s00134 020 06073 8Document7 pagess00134 020 06073 8Andres Rojas JerezNo ratings yet
- J JCRC 2013 11 018Document5 pagesJ JCRC 2013 11 018Andres Rojas JerezNo ratings yet
- Guideline7-GuidelinesforEEGReporting v1Document5 pagesGuideline7-GuidelinesforEEGReporting v1Mannix Gutierrez PonceNo ratings yet
- Ni Hms 472369Document94 pagesNi Hms 472369Andres Rojas JerezNo ratings yet
- J Neulet 2010 03 029Document4 pagesJ Neulet 2010 03 029Andres Rojas JerezNo ratings yet
- JW Guideline Watch 2019Document23 pagesJW Guideline Watch 2019Andres Rojas JerezNo ratings yet
- Iatrogenic Damage To The Mandibular Nerves As AssessedDocument4 pagesIatrogenic Damage To The Mandibular Nerves As AssessedAndres Rojas JerezNo ratings yet
- Epilepsia Lobublo Temporal SND EtmDocument9 pagesEpilepsia Lobublo Temporal SND EtmAndres Rojas JerezNo ratings yet
- Tratado de Psiquiatría Clínica - Psiquiatria - MassachusettsDocument1,139 pagesTratado de Psiquiatría Clínica - Psiquiatria - MassachusettsMarcela100% (2)
- Electroencefalografia Introducción PDFDocument96 pagesElectroencefalografia Introducción PDFMaRianaP.EscalonaNo ratings yet
- Guideline2-GuidelinesforStandardElectrodePositionNomenclature v1Document4 pagesGuideline2-GuidelinesforStandardElectrodePositionNomenclature v1Mannix Gutierrez PonceNo ratings yet
- EEG Normalizado 2017Document8 pagesEEG Normalizado 2017Andres Rojas JerezNo ratings yet
- Guideline6-MinimumTechnicalStandardsforEEGRecordinginSuspectedCerebralDeath v1Document4 pagesGuideline6-MinimumTechnicalStandardsforEEGRecordinginSuspectedCerebralDeath v1Muhammad Imran MirzaNo ratings yet
- 01 - Basic Theory of TCM (Nanjing University of TCM)Document128 pages01 - Basic Theory of TCM (Nanjing University of TCM)Andres Rojas JerezNo ratings yet
- Abnormalities of Masseter Reflex InhibitoryDocument5 pagesAbnormalities of Masseter Reflex InhibitoryAndres Rojas JerezNo ratings yet
- Images-261751AD JW GW Premi 0916 P3Document27 pagesImages-261751AD JW GW Premi 0916 P3Andres Rojas JerezNo ratings yet
- Ophthalmology 2004 Vol (1) .17 Issues 1 ImagingDocument106 pagesOphthalmology 2004 Vol (1) .17 Issues 1 ImagingAndres Rojas JerezNo ratings yet
- JCM Article 1 PDFDocument10 pagesJCM Article 1 PDFAndres Rojas JerezNo ratings yet
- Cranial Nerve V2 - Maxillary Nerve - FRCEM SuccessDocument1 pageCranial Nerve V2 - Maxillary Nerve - FRCEM SuccessJohn CoxNo ratings yet
- Migraine Diagnosis and PathophysiologyDocument11 pagesMigraine Diagnosis and PathophysiologymarthintoriNo ratings yet
- Topical Diagnosis: Department of Anatomy Medical Faculty, Hasanuddin UniversityDocument48 pagesTopical Diagnosis: Department of Anatomy Medical Faculty, Hasanuddin UniversityRey Alwiwikh100% (1)
- Sensation Kinds and Types of Sensory Disturbance Syndromes of LesionDocument67 pagesSensation Kinds and Types of Sensory Disturbance Syndromes of LesionAhmed Adel SaadNo ratings yet
- Cranial Nerves ExamDocument58 pagesCranial Nerves ExamTom JenyonNo ratings yet
- Neuroscience NotesDocument35 pagesNeuroscience NotesAnna Conigrave100% (4)
- Nervous System OverviewDocument29 pagesNervous System OverviewDarla Mitu100% (2)
- Manish Chandra Prabhakar Mgims: 1 Reference-Harrison's Internal Medicine 18th EditionDocument79 pagesManish Chandra Prabhakar Mgims: 1 Reference-Harrison's Internal Medicine 18th EditionManish Chandra PrabhakarNo ratings yet
- Facial Paralysis Reconstruction in Children and Adolescents With Central Nervous System TumorsDocument12 pagesFacial Paralysis Reconstruction in Children and Adolescents With Central Nervous System TumorsCarlos Ageno AlemánNo ratings yet
- CH 6 - Histology and Physiology of The Extraocular Muscles, P. 101-113-EmailDocument13 pagesCH 6 - Histology and Physiology of The Extraocular Muscles, P. 101-113-EmailAmi MisiciNo ratings yet
- InfraTemporal FossaDocument34 pagesInfraTemporal FossaAhmed JawdetNo ratings yet
- Pain ManagementDocument17 pagesPain Managementa bNo ratings yet
- 02whole PDFDocument298 pages02whole PDFpratama wicaksana nugrahaNo ratings yet
- Cranial Nerve V Anatomy and FunctionsDocument76 pagesCranial Nerve V Anatomy and FunctionsAlexAlxNo ratings yet
- Cranial Nerve ExaminationDocument46 pagesCranial Nerve ExaminationKartu KrishnanNo ratings yet
- Trigeminal Nerve FinalDocument101 pagesTrigeminal Nerve FinalShraddha PatilNo ratings yet
- Head and Neck McqsDocument3 pagesHead and Neck McqsRajitha DilhanNo ratings yet
- J Neurosurg Article p1462Document15 pagesJ Neurosurg Article p1462Patus QuakusNo ratings yet
- Bruno BondioliDocument6 pagesBruno BondioliMichellalvarez150No ratings yet
- Cranial Nerve Part 2 (V, VII) : By: Fajri Mohammed (MD)Document51 pagesCranial Nerve Part 2 (V, VII) : By: Fajri Mohammed (MD)abo kooNo ratings yet
- Head and NeckDocument299 pagesHead and NeckDevsya DodiaNo ratings yet
- Cranial Nerves 2010Document25 pagesCranial Nerves 2010Rosa hcNo ratings yet
- Table 1. General Somatic Sensory: Tracts Stimulus Function N1 N2 Decussation N3 N4 Additional InfoDocument8 pagesTable 1. General Somatic Sensory: Tracts Stimulus Function N1 N2 Decussation N3 N4 Additional InfoNicole Villaflor FabicoNo ratings yet
- Micro B - Ascending Tracts SummaryDocument1 pageMicro B - Ascending Tracts SummaryMitchu Tan100% (1)
- Dysphagia Case History: Chart ReviewDocument24 pagesDysphagia Case History: Chart ReviewTiffani Wallace75% (4)
- Physiology of Mastication and Deglutition ExplainedDocument3 pagesPhysiology of Mastication and Deglutition ExplainedAlya Putri KhairaniNo ratings yet
- TMP - 21700-Basic Science Summary For The MRCS-2069613412Document111 pagesTMP - 21700-Basic Science Summary For The MRCS-2069613412Omar Sarahneh100% (5)
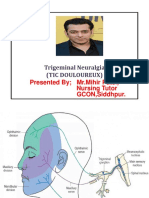
- Trigeminal NeuralgiaDocument15 pagesTrigeminal NeuralgiaMihir Patel75% (4)
- Neurology 4 PDF-mergedDocument358 pagesNeurology 4 PDF-mergedAnuraag YadavNo ratings yet
- The Brain: Muh - Iqbal BasriDocument40 pagesThe Brain: Muh - Iqbal Basrinurul rezki fitrianiazisNo ratings yet