You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Fracture-Dislocation of The Ankle With Fixed Displacement of The Fibula Behind The TibiaDocument4 pagesFracture-Dislocation of The Ankle With Fixed Displacement of The Fibula Behind The TibiaIbnu SyahNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Adductor Canal Block For Postoperative Pain Relief in Knee Surgeries A Review Article 2155 6148 1000578Document4 pagesAdductor Canal Block For Postoperative Pain Relief in Knee Surgeries A Review Article 2155 6148 1000578Ibnu SyahNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Allergy Prevention in The Future of NationDocument43 pagesAllergy Prevention in The Future of NationIbnu SyahNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Impact of Postoperative Pain On Early Ambulation After Hip FractureDocument4 pagesThe Impact of Postoperative Pain On Early Ambulation After Hip FractureIbnu SyahNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Anesthesia & Analgesia-Nov05Document336 pagesAnesthesia & Analgesia-Nov05Ibnu SyahNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Adductor Canal Block For Postoperative Pain Relief in Knee Surgeries A Review Article 2155 6148 1000578Document4 pagesAdductor Canal Block For Postoperative Pain Relief in Knee Surgeries A Review Article 2155 6148 1000578Ibnu SyahNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- TORCH Repro 2012Document44 pagesTORCH Repro 2012Ibnu SyahNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- SKILL LAB LBM 2 Zung Depression Rating ScaleDocument2 pagesSKILL LAB LBM 2 Zung Depression Rating ScaleIbnu SyahNo ratings yet
- JUU Speech by ARDDocument8 pagesJUU Speech by ARDBriliansy MulyantoNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Dwarfism: Navigation Search Dwarf (Germanic Mythology) DwarfDocument15 pagesDwarfism: Navigation Search Dwarf (Germanic Mythology) DwarfManzano JenecaNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Structure of KidneysDocument36 pagesStructure of KidneysunisoldierNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- MBFHI Self AppraisalDocument26 pagesMBFHI Self AppraisalKarz KaraoNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Ability of Prehabilitation To Influence Postoperative Outcome After Intra-Abdominal Operation: A Systematic Review and Meta-AnalysisDocument13 pagesThe Ability of Prehabilitation To Influence Postoperative Outcome After Intra-Abdominal Operation: A Systematic Review and Meta-AnalysisHAriNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Femoral Block Vs Adductor Canal Block: Regional Analgesia For Total Knee ArthroplastyDocument10 pagesFemoral Block Vs Adductor Canal Block: Regional Analgesia For Total Knee ArthroplastyStanford AnesthesiaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Twin-Twin Transfusion Syndrome: Information Leaflet OnDocument8 pagesTwin-Twin Transfusion Syndrome: Information Leaflet Onshona SharupaniNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Or JournalDocument2 pagesOr JournalNathaniel PulidoNo ratings yet
- Royal Crescent Practice Brocher 12pp March 2010 PrintDocument12 pagesRoyal Crescent Practice Brocher 12pp March 2010 PrintyarleyNo ratings yet
- Mallampati 0 2001Document3 pagesMallampati 0 2001Eugenio Daniel Martinez HurtadoNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Diarrhea - Toddlers PDFDocument1 pageDiarrhea - Toddlers PDFNida AwaisNo ratings yet
- The Five Tibetan RitesDocument12 pagesThe Five Tibetan RitesFlorea Eliza100% (1)
- What Is An Intravenous Pyelogram (IVP) ? How Should I Prepare?Document4 pagesWhat Is An Intravenous Pyelogram (IVP) ? How Should I Prepare?vindictive666No ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Thoracic Outlet Syndrome Inferior Thoracic ApertureDocument7 pagesThoracic Outlet Syndrome Inferior Thoracic ApertureerilarchiNo ratings yet
- Diagnosis of Acute Gout: A Clinical Practice Guideline From The American College of PhysiciansDocument8 pagesDiagnosis of Acute Gout: A Clinical Practice Guideline From The American College of PhysiciansRgm UyNo ratings yet
- Essential Intra Natal Care 11aiDocument78 pagesEssential Intra Natal Care 11aiDr Ankush VermaNo ratings yet
- Structural and Dynamic Bases of Hand Surgery by Eduardo Zancolli 1969Document1 pageStructural and Dynamic Bases of Hand Surgery by Eduardo Zancolli 1969khox0% (1)
- Voluson E10 BrochureDocument8 pagesVoluson E10 BrochureJavier VergaraNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
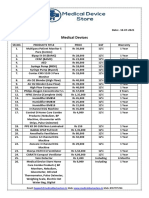
- Medical Device Store Products CatalogueDocument3 pagesMedical Device Store Products CatalogueWasim KhatibNo ratings yet
- Ethical and Legal Issues in Reproductive HealthDocument4 pagesEthical and Legal Issues in Reproductive HealthBianca_P0pNo ratings yet
- 380 (Olive Peart) Lange QA Mammography Examination PDFDocument186 pages380 (Olive Peart) Lange QA Mammography Examination PDFGabriel Callupe100% (1)
- Hemorrhoids: What Are Hemorroids?Document2 pagesHemorrhoids: What Are Hemorroids?Igor DemićNo ratings yet
- English - All Instruction Mannual-20220412-VietnamDocument9 pagesEnglish - All Instruction Mannual-20220412-VietnamHRD Wijaya Mitra HusadaNo ratings yet
- Pneumonperitoneum A Review of Nonsurgical Causes PDFDocument7 pagesPneumonperitoneum A Review of Nonsurgical Causes PDFDellysa Eka Nugraha TNo ratings yet
- Provincial Drug ScheduleDocument16 pagesProvincial Drug ScheduleSamMansuriNo ratings yet
- High School Argumentative Essay TopicsDocument5 pagesHigh School Argumentative Essay Topicslpuaduwhd100% (2)
- CholangiocarcinomaDocument9 pagesCholangiocarcinomaloloalpsheidiNo ratings yet
- ACOG Guidelines For Exercise During PregnancyDocument13 pagesACOG Guidelines For Exercise During Pregnancypptscribid100% (1)
- Anaesthesia Revised A5Document720 pagesAnaesthesia Revised A5barn003100% (1)
- Acupuncture Imaging 31 40 PDFDocument10 pagesAcupuncture Imaging 31 40 PDFmamun31No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)