You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- IMCI Chart Booklet PDFDocument80 pagesIMCI Chart Booklet PDFmikay100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- ImagesDocument32 pagesImagesLing WangNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Lila U GirlsDocument1 pageLila U GirlsNay Ebeye NubaseNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Figure 3-1 Nuclei of Large, Active CellsDocument24 pagesFigure 3-1 Nuclei of Large, Active CellsLeikkaNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- 01Document23 pages01LeikkaNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- IMCI Chart Booklet PDFDocument80 pagesIMCI Chart Booklet PDFmikay100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- CHT Acfa Girls P 3 5Document1 pageCHT Acfa Girls P 3 5Talitha SayoetiNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- CHT Acfa Boys Z 3 5Document1 pageCHT Acfa Boys Z 3 5Rivadin NurwanNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Multifetal PintDocument51 pagesMultifetal PintLeikkaNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- 2.3acongenital Heart Disease VictorDocument16 pages2.3acongenital Heart Disease VictorLeikkaNo ratings yet
- CHT Acfa Boys P 3 5Document1 pageCHT Acfa Boys P 3 5LeikkaNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Lower Genital Tract InfectionsDocument66 pagesLower Genital Tract InfectionsLeikkaNo ratings yet
- Endocrine System - Thyroid Gland - Dr. ValerioDocument8 pagesEndocrine System - Thyroid Gland - Dr. ValerioMelissa SalayogNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- CD 001 Thyroid Diseases Breez E Squad Esguerra 1Document7 pagesCD 001 Thyroid Diseases Breez E Squad Esguerra 1LeikkaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The National Disaster Management ProgramDocument20 pagesThe National Disaster Management ProgramLeikkaNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- 2.4bacquired Heart Diseases (Dr. Latosa) - Feliciano & GigawinDocument10 pages2.4bacquired Heart Diseases (Dr. Latosa) - Feliciano & GigawinLeikkaNo ratings yet
- 3.3medicine 3B Endo Disorders of The Thyroid GlandDocument10 pages3.3medicine 3B Endo Disorders of The Thyroid GlandLeikkaNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- 3.3medicine 3B Endo Disorders of The Thyroid GlandDocument10 pages3.3medicine 3B Endo Disorders of The Thyroid GlandLeikkaNo ratings yet
- TB-Definition of TermsDocument8 pagesTB-Definition of TermsLeikkaNo ratings yet
- 3.3IM 3B - ENDO - THYROID - EjgDocument7 pages3.3IM 3B - ENDO - THYROID - EjgLeikkaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- CD 001 Thyroid Diseases Breez E Squad Esguerra 1Document7 pagesCD 001 Thyroid Diseases Breez E Squad Esguerra 1LeikkaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- LeprosyDocument6 pagesLeprosyLeikkaNo ratings yet
- ReactionDocument3 pagesReactionLeikkaNo ratings yet
- ExtremitiesDocument4 pagesExtremitiesLeikkaNo ratings yet
- LymphedemaLymphedema in A 7Document1 pageLymphedemaLymphedema in A 7LeikkaNo ratings yet
- TB-Intro and StatDocument12 pagesTB-Intro and StatLeikkaNo ratings yet
- Pathophysiology of TuberculosisDocument2 pagesPathophysiology of TuberculosisLeikkaNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Antiespasmódicos - SimeticonaDocument8 pagesAntiespasmódicos - SimeticonaCamilla CristinaNo ratings yet
- CIMS Health Checkup Brochure (English) PDFDocument4 pagesCIMS Health Checkup Brochure (English) PDFVaibhavNo ratings yet
- Isolation 2007Document219 pagesIsolation 2007Jorge CunhaNo ratings yet
- Hypertension in pregnancy-ACOG 2013-1 PDFDocument100 pagesHypertension in pregnancy-ACOG 2013-1 PDFrabinreaganNo ratings yet
- Leriche Fontaine Classification PDFDocument8 pagesLeriche Fontaine Classification PDFCute Clothing StoreNo ratings yet
- Ethics Essential For Usmle Step 1 ExamDocument48 pagesEthics Essential For Usmle Step 1 ExamJunaid AnwarNo ratings yet
- Lecture Note: Health Information Management I (Hit 111)Document27 pagesLecture Note: Health Information Management I (Hit 111)Usman Ahmad TijjaniNo ratings yet
- A Clinical Report On Partial Pulpotomy and Capping With Calcium Hydroxide in Permanent Incisors With Complicated Crown FractureDocument6 pagesA Clinical Report On Partial Pulpotomy and Capping With Calcium Hydroxide in Permanent Incisors With Complicated Crown Fractureroy sepNo ratings yet
- Convocation Medal ListDocument18 pagesConvocation Medal ListVidya SagarNo ratings yet
- DEMENTIADocument42 pagesDEMENTIAputri maharaniNo ratings yet
- How Does Hypnosis Work Ebook Uncommon KnowledgeDocument12 pagesHow Does Hypnosis Work Ebook Uncommon KnowledgeHarsh TripathiNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ATI Week 15Document4 pagesATI Week 15Tee WoodNo ratings yet
- Admission and DischargeDocument3 pagesAdmission and DischargePhilip Jay Braga100% (1)
- Health Optimizing Physical Education 1Document22 pagesHealth Optimizing Physical Education 1Russel MejicoNo ratings yet
- Pemphigus Vulgaris PDFDocument1 pagePemphigus Vulgaris PDFAnonymous PwnuzpY4RNo ratings yet
- Shimla Nursing College Annadale Bai BerbaiDocument17 pagesShimla Nursing College Annadale Bai Berbaigill priyaNo ratings yet
- My New ThesisDocument7 pagesMy New ThesisAlla Yeswanth Dilip KumarNo ratings yet
- Residency Prog CanadaDocument116 pagesResidency Prog Canadahswami20037730No ratings yet
- Treatments For OsteoporosisDocument2 pagesTreatments For Osteoporosisawaw90No ratings yet
- EpidemiologyDocument52 pagesEpidemiologyasdfsNo ratings yet
- Infection Control Practice On Vital Signs Equipment: A Survey Among Senior Nursing Students in Iloilo City, PhilippinesDocument7 pagesInfection Control Practice On Vital Signs Equipment: A Survey Among Senior Nursing Students in Iloilo City, PhilippinesRyan Michael OducadoNo ratings yet
- MDHA Write-Up For Prospective StudentsDocument1 pageMDHA Write-Up For Prospective StudentsprashantNo ratings yet
- Introduction To Epidemiology & Public Health: Dr. Munibullah LecturerDocument22 pagesIntroduction To Epidemiology & Public Health: Dr. Munibullah LecturerIbrar Faisal0% (1)
- AYUSH Project ReportDocument3 pagesAYUSH Project ReportPaulNo ratings yet
- Reading Comprehension Exercise, May 3rdDocument3 pagesReading Comprehension Exercise, May 3rdPalupi Salwa BerliantiNo ratings yet
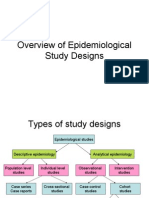
- Overview of Epidemiological Study DesignsDocument16 pagesOverview of Epidemiological Study DesignsLakshmi Seth100% (2)
- The Carcinosin Drug Picture - Dr. FoubisterDocument34 pagesThe Carcinosin Drug Picture - Dr. FoubisterRogelio VillegasNo ratings yet
- The Aspects of Gene TherapyDocument15 pagesThe Aspects of Gene TherapyLaleth Mendoza Ojales0% (1)
- Maharshi Dayanand University RohtakDocument3 pagesMaharshi Dayanand University RohtakMukesh BishtNo ratings yet
- Post Term PregnancyDocument22 pagesPost Term PregnancyDarianne HernandezNo ratings yet
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (6)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (26)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (404)