You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Rabies SurveillanceDocument4 pagesRabies SurveillanceResti Purnama SariNo ratings yet
- PEP Prophylaxis Guideline 15 12 2014 PDFDocument27 pagesPEP Prophylaxis Guideline 15 12 2014 PDFjessicacookNo ratings yet
- WHO Rabies GuideDocument24 pagesWHO Rabies Guidemuzicka9No ratings yet
- PEP Prophylaxis Guidelines June10Document21 pagesPEP Prophylaxis Guidelines June10Mary Hope A. LimaNo ratings yet
- PH GR Rabies 20 Jan 201010 AmDocument62 pagesPH GR Rabies 20 Jan 201010 AmPatricia EngalladoNo ratings yet
- PH GR Rabies 20 Jan 201010 AmDocument62 pagesPH GR Rabies 20 Jan 201010 AmPatricia EngalladoNo ratings yet
- PH GR Rabies 20 Jan 201010 AmDocument62 pagesPH GR Rabies 20 Jan 201010 AmPatricia EngalladoNo ratings yet
- Rabies SurveillanceDocument4 pagesRabies SurveillanceResti Purnama SariNo ratings yet
- Penegakan Diagnosis Anemic Heart DiseaseDocument3 pagesPenegakan Diagnosis Anemic Heart DiseasejessicacookNo ratings yet
- E-Journal GJMR (C) Vol 15 Issue 2 PDFDocument55 pagesE-Journal GJMR (C) Vol 15 Issue 2 PDFjessicacookNo ratings yet
- NTDT TIF Guidelines PDFDocument120 pagesNTDT TIF Guidelines PDFjessicacookNo ratings yet
- Guidelines For The Clinical Care of Patients With Thalassemia in CanadaDocument84 pagesGuidelines For The Clinical Care of Patients With Thalassemia in Canadaalihos93No ratings yet
- P2 - Therapy PDFDocument12 pagesP2 - Therapy PDFElizabeth SniderNo ratings yet
- Clin Chim Acta 2009Document8 pagesClin Chim Acta 2009Daniel MejiaNo ratings yet
- Hemorrhoids Pathophysiology To TreatmentDocument9 pagesHemorrhoids Pathophysiology To TreatmentKen CheungNo ratings yet
- EmCheckTest PDFDocument11 pagesEmCheckTest PDFjessicacookNo ratings yet
- Wa0000 PDFDocument28 pagesWa0000 PDFUchi Erian Febriana IINo ratings yet
- AnestesiDocument11 pagesAnestesijessicacookNo ratings yet
- BronkiolitisDocument21 pagesBronkiolitisRaditya Rangga PratamaNo ratings yet
- Clin Infect Dis.-2004-Wilson-1150-8 PDFDocument9 pagesClin Infect Dis.-2004-Wilson-1150-8 PDFjessicacookNo ratings yet
- 1800 10330 1 PB PDFDocument1 page1800 10330 1 PB PDFjessicacookNo ratings yet
- 6644 12978 1 SMDocument10 pages6644 12978 1 SMjessicacookNo ratings yet
- Hemoroid JurnalDocument7 pagesHemoroid JurnalAsti HaryaniNo ratings yet
- Specialists in Reproductive Medicine & Surgery, P.A.: Definition: SchedulingDocument3 pagesSpecialists in Reproductive Medicine & Surgery, P.A.: Definition: SchedulingjessicacookNo ratings yet
- Diagnosis and Treatment of Urinary Tract Infections in ChildrenDocument1 pageDiagnosis and Treatment of Urinary Tract Infections in ChildrenjessicacookNo ratings yet
- Diagnosis and Treatment of Urinary Tract Infections in ChildrenDocument1 pageDiagnosis and Treatment of Urinary Tract Infections in ChildrenjessicacookNo ratings yet
- Batuk Efektif PDFDocument7 pagesBatuk Efektif PDFkhamidaNo ratings yet
- Clin Pediatr 2012 Burgos 7 16Document11 pagesClin Pediatr 2012 Burgos 7 16jessicacookNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- GrandEsta - Double Eyelid Surgery PDFDocument2 pagesGrandEsta - Double Eyelid Surgery PDFaniyaNo ratings yet
- Script For Demo TeachingDocument9 pagesScript For Demo TeachingDindz SurioNo ratings yet
- F A T City Workshop NotesDocument3 pagesF A T City Workshop Notesapi-295119035No ratings yet
- Project Report: Eveplus Web PortalDocument47 pagesProject Report: Eveplus Web Portaljas121No ratings yet
- Mark Scheme (Final) January 2020Document16 pagesMark Scheme (Final) January 2020aqib ameerNo ratings yet
- Malaria SymptomsDocument3 pagesMalaria SymptomsShaula de OcampoNo ratings yet
- Indonesian High School Student Motivational Orientations For Learning English As A Foreign LanguageDocument18 pagesIndonesian High School Student Motivational Orientations For Learning English As A Foreign LanguageAlberth DalopeNo ratings yet
- Swimming Pool - PWTAG CodeofPractice1.13v5 - 000Document58 pagesSwimming Pool - PWTAG CodeofPractice1.13v5 - 000Vin BdsNo ratings yet
- Soal Ujian Tengah Semester Genap Sma Islam Diponegoro Surakarta TAHUN PELAJARAN 2020/2021Document5 pagesSoal Ujian Tengah Semester Genap Sma Islam Diponegoro Surakarta TAHUN PELAJARAN 2020/2021Dian OctavianiNo ratings yet
- Songs of KabirDocument342 pagesSongs of KabirSant MatNo ratings yet
- Infinitives or Gerunds PDFDocument2 pagesInfinitives or Gerunds PDFRosa 06No ratings yet
- Cayman Islands National Youth Policy September 2000Document111 pagesCayman Islands National Youth Policy September 2000Kyler GreenwayNo ratings yet
- The Interplay of Religion and PoliticsDocument10 pagesThe Interplay of Religion and PoliticsThompson mercyNo ratings yet
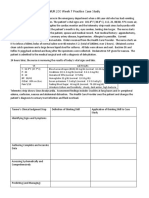
- NUR 200 Week 7 Practice Case StudyDocument2 pagesNUR 200 Week 7 Practice Case StudyJB NicoleNo ratings yet
- t10 2010 Jun QDocument10 pagest10 2010 Jun QAjay TakiarNo ratings yet
- Ethiopia FormularyDocument543 pagesEthiopia Formularyabrham100% (1)
- Icmap Newsletter June 2017Document7 pagesIcmap Newsletter June 2017GoopNo ratings yet
- Reaction PaperDocument3 pagesReaction PaperPatrick Ramos80% (15)
- Business Intelligence in RetailDocument21 pagesBusiness Intelligence in RetailGaurav Kumar100% (1)
- mc96 97 01feb - PsDocument182 pagesmc96 97 01feb - PsMohammed Rizwan AliNo ratings yet
- Sancticity AllDocument21 pagesSancticity AllJames DeHart0% (1)
- Tips On Being A Successful StudentDocument2 pagesTips On Being A Successful Studentshimbir100% (3)
- Chap 9 Special Rules of Court On ADR Ver 1 PDFDocument8 pagesChap 9 Special Rules of Court On ADR Ver 1 PDFambahomoNo ratings yet
- Math 209: Numerical AnalysisDocument31 pagesMath 209: Numerical AnalysisKish NvsNo ratings yet
- 1 Patient Assessment Form.Document3 pages1 Patient Assessment Form.Aina HaravataNo ratings yet
- Eyewitness Bloody Sunday PDFDocument2 pagesEyewitness Bloody Sunday PDFKatie0% (1)
- Gamma Ray Interaction With Matter: A) Primary InteractionsDocument10 pagesGamma Ray Interaction With Matter: A) Primary InteractionsDr-naser MahmoudNo ratings yet
- Module 7 - Prob D-E Valuation and Concepts AnswersDocument3 pagesModule 7 - Prob D-E Valuation and Concepts Answersvenice cambryNo ratings yet
- 2.2 Push and Pull Sources of InnovationDocument16 pages2.2 Push and Pull Sources of Innovationbclarke113No ratings yet
- Geoland InProcessingCenterDocument50 pagesGeoland InProcessingCenterjrtnNo ratings yet