You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Medsurg Cardio Ana&PhysioDocument6 pagesMedsurg Cardio Ana&Physiorabsibala80% (10)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Divine Intervention Episode 22 Obgyn Shelf Review PDFDocument167 pagesDivine Intervention Episode 22 Obgyn Shelf Review PDFSwisskelly1100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Anti-Drug Campaign SpeechDocument2 pagesAnti-Drug Campaign SpeechGracel Gonzaga Eviota91% (11)
- Psychological First Aid-A Training GuideDocument8 pagesPsychological First Aid-A Training Guidejprewittdiaz100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Anaesthesia Q Review 2014Document33 pagesAnaesthesia Q Review 2014ChandanJha100% (8)
- Basic Sciences in Ophthalmology - 9788184486087-EmailDocument446 pagesBasic Sciences in Ophthalmology - 9788184486087-EmailwulanfarichahNo ratings yet
- Angel EssenceDocument23 pagesAngel EssenceShivani Manchanda50% (2)
- MelatoninaDocument32 pagesMelatoninaCodrut GeorgescuNo ratings yet
- Chart FastingDocument1 pageChart FastingGary S75% (4)
- Set 5Document18 pagesSet 5Dick Morgan FerrerNo ratings yet
- Intestinal DisordersDocument11 pagesIntestinal DisorderspulmonologistNo ratings yet
- A Multi-Disciplinary Approach To Class III Therapy Using The Delta Force and ALF Appliances in Conjunction With Terminal Arch ExtractionsDocument4 pagesA Multi-Disciplinary Approach To Class III Therapy Using The Delta Force and ALF Appliances in Conjunction With Terminal Arch ExtractionsOrtho OrganizersNo ratings yet
- Hahn, R. 1995. Sickness and Healing - An Anthropological Perspective. Chap 4 - The Role of Society and Culture in Sickness and HealingDocument24 pagesHahn, R. 1995. Sickness and Healing - An Anthropological Perspective. Chap 4 - The Role of Society and Culture in Sickness and HealingJenny Gill67% (3)
- Ovarian Cyst AcogDocument2 pagesOvarian Cyst AcogDyah Nuriisa ANo ratings yet
- Khromov Y. 1000Document1 pageKhromov Y. 1000wulanfarichahNo ratings yet
- Indikasi Preterm LaborDocument5 pagesIndikasi Preterm LaborGenio RachmadanaNo ratings yet
- Ebm Kista BartolinDocument3 pagesEbm Kista BartolinwulanfarichahNo ratings yet
- Like Colonic InjuriesDocument2 pagesLike Colonic InjurieswulanfarichahNo ratings yet
- Ebm Kista BartolinDocument3 pagesEbm Kista BartolinwulanfarichahNo ratings yet
- Ebm HegDocument5 pagesEbm HegwulanfarichahNo ratings yet
- Management of Breech PresentationDocument13 pagesManagement of Breech Presentationdr.Hansen.SH100% (1)
- Anal SacDocument4 pagesAnal SacwulanfarichahNo ratings yet
- Prenatal 03 0015Document3 pagesPrenatal 03 0015Al MubartaNo ratings yet
- Blunt and Penetrating Injuries To The Anus and Rectum Are UncommonDocument7 pagesBlunt and Penetrating Injuries To The Anus and Rectum Are UncommonwulanfarichahNo ratings yet
- Management of Breech PresentationDocument13 pagesManagement of Breech Presentationdr.Hansen.SH100% (1)
- Ebm OligohidramnionDocument4 pagesEbm OligohidramnionwulanfarichahNo ratings yet
- Maternal Complications Linked to Prolonged Second Stage LabourDocument9 pagesMaternal Complications Linked to Prolonged Second Stage LabourwulanfarichahNo ratings yet
- Maternal Complications Linked to Prolonged Second Stage LabourDocument9 pagesMaternal Complications Linked to Prolonged Second Stage LabourwulanfarichahNo ratings yet
- Intrauterine Ballon Tamponade For The Control of PostpartumDocument6 pagesIntrauterine Ballon Tamponade For The Control of PostpartumwulanfarichahNo ratings yet
- Care of The Patient With Anorectal TraumaDocument5 pagesCare of The Patient With Anorectal TraumawulanfarichahNo ratings yet
- Co 630Document4 pagesCo 630wulanfarichahNo ratings yet
- Screening For Thyroid: Disorders in Pregnancy With TSH EstimationDocument6 pagesScreening For Thyroid: Disorders in Pregnancy With TSH EstimationwulanfarichahNo ratings yet
- Numerous Traumatic Events Can Result in Disruption of TheDocument14 pagesNumerous Traumatic Events Can Result in Disruption of ThewulanfarichahNo ratings yet
- Indikasi Preterm LaborDocument5 pagesIndikasi Preterm LaborGenio RachmadanaNo ratings yet
- Indikasi Preterm LaborDocument5 pagesIndikasi Preterm LaborGenio RachmadanaNo ratings yet
- 89 1426835435Document7 pages89 1426835435wulanfarichahNo ratings yet
- 89 1448294923Document4 pages89 1448294923wulanfarichahNo ratings yet
- 89 1421585163Document6 pages89 1421585163wulanfarichahNo ratings yet
- 89 1452343924Document5 pages89 1452343924wulanfarichahNo ratings yet
- 6.3.9 AAST Organ Injury - RectumDocument1 page6.3.9 AAST Organ Injury - RectumwulanfarichahNo ratings yet
- ANORECTAL INJURY GUIDELINES IN CHILDRENDocument2 pagesANORECTAL INJURY GUIDELINES IN CHILDRENwulanfarichahNo ratings yet
- Dialog EFN2 Sudarmi 30140114040Document2 pagesDialog EFN2 Sudarmi 30140114040sudarmiNo ratings yet
- Comprehensive Review On Endonasal Endoscopic SinusDocument108 pagesComprehensive Review On Endonasal Endoscopic SinusHossam Elden Helmy HaridyNo ratings yet
- Chapter 3 NotesDocument10 pagesChapter 3 Notesmjamie12345No ratings yet
- Illness BehaviorDocument11 pagesIllness BehaviorRubelleMicahCagampangSapongNo ratings yet
- Lab Technician Resume TitleDocument1 pageLab Technician Resume TitleSilvio DTNo ratings yet
- Best of The Best 2013 - Winner's SectionDocument38 pagesBest of The Best 2013 - Winner's SectionTrent SpoffordNo ratings yet
- Stroe Be 2017Document27 pagesStroe Be 2017Iris Moreno R100% (1)
- DVT Formation and TreatmentDocument24 pagesDVT Formation and TreatmentdinafiniNo ratings yet
- NANDA DefinitionDocument5 pagesNANDA DefinitionAngel_Liboon_388No ratings yet
- Alzheimer's Research PaperDocument5 pagesAlzheimer's Research PaperJosh BarnutNo ratings yet
- Ongoing Professional Practice Evaluation (Oppe) : Administrative Policies and ProceduresDocument5 pagesOngoing Professional Practice Evaluation (Oppe) : Administrative Policies and ProceduresTary BaruNo ratings yet
- Revised Kanda NCPDocument3 pagesRevised Kanda NCPhaxa yzaNo ratings yet
- Caries Predication, Risk Assessment and Treatment PlanningDocument74 pagesCaries Predication, Risk Assessment and Treatment PlanningmohammadNo ratings yet
- Mental Health Nursing RequirementsDocument5 pagesMental Health Nursing RequirementsNuay LaoNo ratings yet
- Applying Client-Centred Guidelines to Pediatric OTDocument7 pagesApplying Client-Centred Guidelines to Pediatric OTRaphael AguiarNo ratings yet
- Trigger Finger PostopDocument2 pagesTrigger Finger PostopNandaSuryaWijayaNo ratings yet
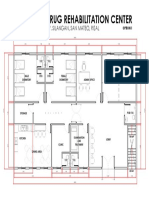
- Proposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalDocument1 pageProposed Drug Rehabilitation Center: Monterey Sudb., Brgy. Silangan, San Mateo, RizalJonathan MazonNo ratings yet