You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Using Evidence On Violence and InjuryDocument14 pagesUsing Evidence On Violence and InjurySifra Turu AlloNo ratings yet
- Sifra Jurnal 2Document5 pagesSifra Jurnal 2Sifra Turu AlloNo ratings yet
- 00e Editorial - 362 364Document3 pages00e Editorial - 362 364Sifra Turu AlloNo ratings yet
- Factors Associated With Hepatitis C Seropositivity in People Living With HIVDocument7 pagesFactors Associated With Hepatitis C Seropositivity in People Living With HIVSifra Turu AlloNo ratings yet
- (696557968) Sifra JurnalDocument9 pages(696557968) Sifra JurnalSifra Turu AlloNo ratings yet
- Factors Associated With Hepatitis C Seropositivity in People Living With HIVDocument7 pagesFactors Associated With Hepatitis C Seropositivity in People Living With HIVSifra Turu AlloNo ratings yet
- Depression Among Women in California and Border RegionDocument10 pagesDepression Among Women in California and Border RegionSifra Turu AlloNo ratings yet
- 00c Editorial - 355 358Document4 pages00c Editorial - 355 358Sifra Turu AlloNo ratings yet
- Tuberculosis Transmission Across The United States-Mexico BorderDocument4 pagesTuberculosis Transmission Across The United States-Mexico BorderSifra Turu AlloNo ratings yet
- Tuberculosis Transmission Across The United States-Mexico BorderDocument4 pagesTuberculosis Transmission Across The United States-Mexico BorderSifra Turu AlloNo ratings yet
- 14 C Neuropsychological Assessment in ChildrenDocument7 pages14 C Neuropsychological Assessment in ChildrenSifra Turu AlloNo ratings yet
- Use Only: Violence in Childhood-Onset SchizophreniaDocument5 pagesUse Only: Violence in Childhood-Onset SchizophreniaSifra Turu AlloNo ratings yet
- 14 C Neuropsychological Assessment in ChildrenDocument7 pages14 C Neuropsychological Assessment in ChildrenSifra Turu AlloNo ratings yet
- Forlap DiktiDocument1 pageForlap DiktiSifra Turu AlloNo ratings yet
- Tuberculosis Transmission Across The United States-Mexico BorderDocument4 pagesTuberculosis Transmission Across The United States-Mexico BorderSifra Turu AlloNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Covid-19 Pandemic and Its Impacts On Micro Small and Medium Enterprises of AssamDocument8 pagesCovid-19 Pandemic and Its Impacts On Micro Small and Medium Enterprises of AssamIJAR JOURNALNo ratings yet
- Coronavirus (COVID-19) Testing - Statistics and Research - Our World in DataDocument89 pagesCoronavirus (COVID-19) Testing - Statistics and Research - Our World in Datahah266611No ratings yet
- Non-Hodgkin'S Lymphoma: Oliveros Francis!!!!!!!!!!!!!!!!!Document48 pagesNon-Hodgkin'S Lymphoma: Oliveros Francis!!!!!!!!!!!!!!!!!francis00090No ratings yet
- General Pathology Practical Exam Renal PathologyDocument16 pagesGeneral Pathology Practical Exam Renal PathologyCherry RahimaNo ratings yet
- Review of Related Literature Covid-19 Classification: Rhinolophus AffinisDocument7 pagesReview of Related Literature Covid-19 Classification: Rhinolophus Affinissamiza1122No ratings yet
- 23 Avian Leukosis Complex 1Document14 pages23 Avian Leukosis Complex 1Aqib HussainNo ratings yet
- Computer-Based English Proficiency Test AdvisoryDocument7 pagesComputer-Based English Proficiency Test AdvisoryJoyce CarilloNo ratings yet
- 10 Healty Gateways Info For Ships To Prepare For COVID-19 PDFDocument16 pages10 Healty Gateways Info For Ships To Prepare For COVID-19 PDFDennis VolodchenkoNo ratings yet
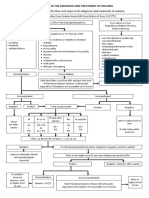
- Algorithm in The Diagnosis and Treatment of MalariaDocument1 pageAlgorithm in The Diagnosis and Treatment of MalariaPearl Monette Cedeño AngNo ratings yet
- Managing Hypertension and Rheumatoid ArthritisDocument2 pagesManaging Hypertension and Rheumatoid ArthritisKristinelou Marie ReynaNo ratings yet
- Initial Patient Assessment in OpdDocument4 pagesInitial Patient Assessment in OpdLokender Goyal100% (1)
- Measles Outbreak Spreads in BarangayDocument2 pagesMeasles Outbreak Spreads in BarangayAhmed-Adhiem Bahjin KamlianNo ratings yet
- What Is SyphilisDocument12 pagesWhat Is SyphilisBheru LalNo ratings yet
- Department of Molecular Virology: COVID-19 (Corona) VirusDocument1 pageDepartment of Molecular Virology: COVID-19 (Corona) VirusMuhammad AreebNo ratings yet
- DR Harikrishna - Management of Diabetic FootDocument89 pagesDR Harikrishna - Management of Diabetic FootAdrian Lim100% (2)
- HISTORY AND PHYSICAL EXAMINATION (Putul)Document2 pagesHISTORY AND PHYSICAL EXAMINATION (Putul)Reshma Francis100% (1)
- TORCH in PregnancyDocument63 pagesTORCH in PregnancyKinjal VasavaNo ratings yet
- Guideline MERS Management in Malaysia, 2023Document123 pagesGuideline MERS Management in Malaysia, 2023Nezly IderusNo ratings yet
- Gastroenteritis and Enterocolitis PBL ObjectivesDocument5 pagesGastroenteritis and Enterocolitis PBL ObjectivesPaul A IBattledaily ScavellaNo ratings yet
- Infections of The Eyes and The Central Nervous System by Dr. Joan E. CerradaDocument68 pagesInfections of The Eyes and The Central Nervous System by Dr. Joan E. CerradaMonique BorresNo ratings yet
- Vaccination of Healthcare WorkersDocument16 pagesVaccination of Healthcare WorkersBenjamin RuotiNo ratings yet
- Kawasaki DiseaseDocument41 pagesKawasaki DiseaseWuryan Dewi Mftahtyas ArumNo ratings yet
- Literature ReviewDocument6 pagesLiterature Reviewapi-563243682No ratings yet
- Epidemiology - ReportDocument9 pagesEpidemiology - ReportIsabel HernandezNo ratings yet
- (CGPT) B11M4.1Document12 pages(CGPT) B11M4.1adriennemartha.barrientosNo ratings yet
- Hashimoto's Thyroiditis InfographicDocument1 pageHashimoto's Thyroiditis InfographicCleoNo ratings yet
- WIL - English Does Work 7 Cronica WRITINGDocument2 pagesWIL - English Does Work 7 Cronica WRITINGwilbert edill rodriguez martinez50% (2)
- Polymyalgia Rheumatic Symptoms Diagnosis and TreatmentDocument2 pagesPolymyalgia Rheumatic Symptoms Diagnosis and TreatmentHas SimNo ratings yet
- Icicipru Smart Health LeafletDocument8 pagesIcicipru Smart Health LeafletKuldip BarmanNo ratings yet
- Framingham Data Famous Cohort Study of 5209 Subjects From Framingham MADocument2 pagesFramingham Data Famous Cohort Study of 5209 Subjects From Framingham MAEdwin Johny Asnate SalazarNo ratings yet