You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Herman Gendered Restrooms and Minority Stress June 2013Document16 pagesHerman Gendered Restrooms and Minority Stress June 2013Julisa FernandezNo ratings yet
- Campus Sexual Violence - Statistics - RAINNDocument6 pagesCampus Sexual Violence - Statistics - RAINNJulisa FernandezNo ratings yet
- Hands Only CPRDocument7 pagesHands Only CPRJulisa FernandezNo ratings yet
- Validate Rendering Fidelity by Referencing The 1 MV ECG Calibration SignalsDocument1 pageValidate Rendering Fidelity by Referencing The 1 MV ECG Calibration SignalsJulisa FernandezNo ratings yet
- Disrythmia Recognition ACLS ASHIDocument127 pagesDisrythmia Recognition ACLS ASHIJulisa FernandezNo ratings yet
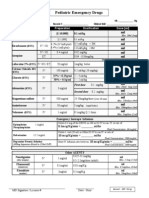
- PediatricResuscMeds HOPUDocument1 pagePediatricResuscMeds HOPUJulisa FernandezNo ratings yet
- Technical Search Considerations - Listening TechniquesDocument41 pagesTechnical Search Considerations - Listening TechniquesJulisa FernandezNo ratings yet
- Technical Search Considerations - Search MarkingsDocument24 pagesTechnical Search Considerations - Search MarkingsJulisa FernandezNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Brachial Plexus InjuryDocument10 pagesBrachial Plexus InjurySanditya FadliNo ratings yet
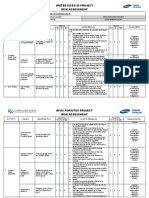
- Apoc Risk Assessment Format - Sesa-Bfim-Ra-Cs-001Document11 pagesApoc Risk Assessment Format - Sesa-Bfim-Ra-Cs-001Abdul WasayNo ratings yet
- Ma Gui Ba Gua Sample Exercise DocumentDocument14 pagesMa Gui Ba Gua Sample Exercise Documentshmoopiebear50% (2)
- Inbound 7714832539582663562Document17 pagesInbound 7714832539582663562Julesbon ParsaliganNo ratings yet
- Maclin SuitDocument5 pagesMaclin Suitnicholas.phillipsNo ratings yet
- 4.b. Medical For Athletes 2Document2 pages4.b. Medical For Athletes 2Mark Era Acson De LunaNo ratings yet
- Pe & Health 6-25-14 PDFDocument432 pagesPe & Health 6-25-14 PDFRomeo D Belnas0% (1)
- Peripheral Nervous System NotesDocument9 pagesPeripheral Nervous System NotesSaoirseNo ratings yet
- Easy Care 2100 User ManualDocument8 pagesEasy Care 2100 User ManualJim BurkeNo ratings yet
- Cerebral HemorrhageDocument10 pagesCerebral HemorrhageJayd Lorenz Vicente ChuanNo ratings yet
- Pathophysiology: A Clinical Approach (2nd Ed.) - Braun Anderson (Chapter 3)Document8 pagesPathophysiology: A Clinical Approach (2nd Ed.) - Braun Anderson (Chapter 3)Mcat NotensionNo ratings yet
- Resume "Something The Lord Made"Document2 pagesResume "Something The Lord Made"Jennifer OngkoNo ratings yet
- Assessment and Management of Unconscious PatientDocument10 pagesAssessment and Management of Unconscious PatientDebasis SahooNo ratings yet
- Chymoral PlusDocument3 pagesChymoral PlusNeha SureshNo ratings yet
- Muscle Activity During The Gait CycleDocument3 pagesMuscle Activity During The Gait CycleMarjorie Walker100% (1)
- Susan Aikens Vs BBC Worldwide Reality Productions (Life Below Zero)Document32 pagesSusan Aikens Vs BBC Worldwide Reality Productions (Life Below Zero)Kyle Hopkins100% (1)
- M/DN MIS Intramedullary Femoral Fixation Surgical TechniqueDocument32 pagesM/DN MIS Intramedullary Femoral Fixation Surgical TechniqueVamby SabidoNo ratings yet
- Damage Control Orthopaedics (DC O: Presented by Specialist of Orthopedic& Traumatology Al-Mahmoudia General HospitalDocument52 pagesDamage Control Orthopaedics (DC O: Presented by Specialist of Orthopedic& Traumatology Al-Mahmoudia General HospitalpaswordnyalupaNo ratings yet
- Flail Chest MP Shah - CcuDocument29 pagesFlail Chest MP Shah - CcuMARTINNo ratings yet
- Gravaboi Codes and NumbersDocument18 pagesGravaboi Codes and NumbersHenrii Arias0% (1)
- Blyton Enid Now For A Story 1948Document193 pagesBlyton Enid Now For A Story 1948athinapolos100% (1)
- Autologous Platelet-Rich Plasma inDocument6 pagesAutologous Platelet-Rich Plasma innoor hidayahNo ratings yet
- Spinal Cord InjuriesDocument17 pagesSpinal Cord InjuriesspinalcordNo ratings yet
- International General Certificate Candidate's Observation Sheet Igc3 - The Health and Safety Practical ApplicationDocument7 pagesInternational General Certificate Candidate's Observation Sheet Igc3 - The Health and Safety Practical Applicationsubhanmusadiq60% (10)
- Spartacus 2x05 - ReckoningDocument52 pagesSpartacus 2x05 - ReckoningJavier de PascualNo ratings yet
- Manual of Neurologic TherapeuticsDocument534 pagesManual of Neurologic TherapeuticsDefault User100% (1)
- The Girl Who Would Be King Chapters 15 16Document6 pagesThe Girl Who Would Be King Chapters 15 16Waddle DeeNo ratings yet
- Case Study On Open Tibial FractureDocument48 pagesCase Study On Open Tibial FractureOmotosho AlexNo ratings yet
- People v. Dalag y Custodio 402 SCRA 254 PDFDocument27 pagesPeople v. Dalag y Custodio 402 SCRA 254 PDFfelix camerinoNo ratings yet
- PLC InjuryDocument5 pagesPLC InjuryTeng HanNo ratings yet