You might also like
- EW 14 Day 1500 Calorie Meal Plan 0Document5 pagesEW 14 Day 1500 Calorie Meal Plan 0Martha Patricia López PimentelNo ratings yet
- Sensory Diet Template and Activities 1Document6 pagesSensory Diet Template and Activities 1Martha Patricia López Pimentel100% (2)
- Sensory Ideas For Small SpacesDocument1 pageSensory Ideas For Small SpacesMartha Patricia López PimentelNo ratings yet
- Reverse Diet and Muscle Growth GuideDocument41 pagesReverse Diet and Muscle Growth Guider.marchesettiNo ratings yet
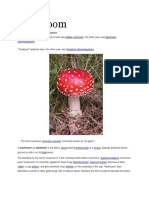
- Mushroom: From Wikipedia, The Free EncyclopediaDocument18 pagesMushroom: From Wikipedia, The Free EncyclopediaErin LeahyNo ratings yet
- OT Grooming Nail TrimmingDocument2 pagesOT Grooming Nail TrimmingMartha Patricia López PimentelNo ratings yet
- Chicken's MoltingDocument11 pagesChicken's MoltingKhaira Fani100% (1)
- 13 Super Food Elixirs V2Document27 pages13 Super Food Elixirs V2igor petrovski98% (48)
- Paleo DessertsDocument273 pagesPaleo Dessertstuan Vladimir100% (3)
- Hyperkalemia PDFDocument1 pageHyperkalemia PDFHaidy JanceNo ratings yet
- ASPEN Enteral Nutrition Handbook, Second EditionDocument468 pagesASPEN Enteral Nutrition Handbook, Second EditionLeticia Granados100% (3)
- Reflexes Check-List Possible Long-Term EffectsDocument6 pagesReflexes Check-List Possible Long-Term EffectsMartha Patricia López PimentelNo ratings yet
- OT Grooming Bath TimeDocument3 pagesOT Grooming Bath TimeMartha Patricia López PimentelNo ratings yet
- Advanced Body of F.I.R.E PDFDocument69 pagesAdvanced Body of F.I.R.E PDFSimon ROBITAILLE100% (1)
- Weight Set-Point Theory Presentation - Laura BaumanDocument17 pagesWeight Set-Point Theory Presentation - Laura BaumanLaura Bauman100% (1)
- Endocrine System MCQDocument19 pagesEndocrine System MCQBijay Kumar MahatoNo ratings yet
- Peer and Family Influence in Eating Disorders - A Meta-AnalysisDocument8 pagesPeer and Family Influence in Eating Disorders - A Meta-AnalysisRose MoralesNo ratings yet
- CPHN Long ExamDocument13 pagesCPHN Long ExamJohn Michael MacabentaNo ratings yet
- Pathophysiology CholecystitisDocument4 pagesPathophysiology CholecystitiskikaycutieNo ratings yet
- HormonesDocument31 pagesHormonestuvvacNo ratings yet
- Milk Products Regulations Sri LankaDocument20 pagesMilk Products Regulations Sri Lankaiwan100% (1)
- Identifying AdverbsDocument2 pagesIdentifying AdverbsMartha Patricia López Pimentel0% (1)
- Keluarga 2..12966 - 2016 - Article - 393-1Document12 pagesKeluarga 2..12966 - 2016 - Article - 393-1Aisyah GirindraNo ratings yet
- Journal 2Document10 pagesJournal 2api-273084987No ratings yet
- XSocial Media, Thin Ideal, Body Dissatisfaction and Disordered Eating Attitudes An Exploratory AnalysisDocument16 pagesXSocial Media, Thin Ideal, Body Dissatisfaction and Disordered Eating Attitudes An Exploratory AnalysisMaría De Guadalupe ToralesNo ratings yet
- Psychosocial and Familial Impairment Among Overweight Youth With Social ProblemsDocument8 pagesPsychosocial and Familial Impairment Among Overweight Youth With Social Problemsmutiara hapkaNo ratings yet
- Mapping and Visualisation Software Tools A ReviewDocument22 pagesMapping and Visualisation Software Tools A ReviewTatiana MachadoNo ratings yet
- Reversing The Trend of Childhood ObesityDocument6 pagesReversing The Trend of Childhood ObesitySharon V.No ratings yet
- Utilizing Social Action Approaches To Address Childhood Obesity in The United StatesDocument18 pagesUtilizing Social Action Approaches To Address Childhood Obesity in The United StatesAJ Brian MundiaNo ratings yet
- Qual 2Document13 pagesQual 2api-577249675No ratings yet
- Running Head: PROGRAM DESIGN: Childhood Obesity: Risk Factors & ImplicationsDocument34 pagesRunning Head: PROGRAM DESIGN: Childhood Obesity: Risk Factors & Implicationsapi-338691074No ratings yet
- CheeeeDocument9 pagesCheeeeNet Chee AlampayNo ratings yet
- Is Obesity in Australia A Trouble or An Issue?Document4 pagesIs Obesity in Australia A Trouble or An Issue?gabNo ratings yet
- PCD 12 E42Document11 pagesPCD 12 E42api-326476970No ratings yet
- Prevention ObesityDocument13 pagesPrevention ObesityDaira QuinteroNo ratings yet
- Weight Shame, Social Connection, and Depressive Symptoms in Late AdolescenceDocument12 pagesWeight Shame, Social Connection, and Depressive Symptoms in Late Adolescencenel nuggetNo ratings yet
- DeSmet (2014)Document12 pagesDeSmet (2014)FlorinaNo ratings yet
- The Effect of Social Cognitive Theory BaDocument9 pagesThe Effect of Social Cognitive Theory BaJulivert JasminNo ratings yet
- 1471 2458 13 900 Iscole PDFDocument13 pages1471 2458 13 900 Iscole PDFSIRIUS RTNo ratings yet
- Social Media Affinity and Eating HabitsDocument2 pagesSocial Media Affinity and Eating HabitsKrimson BomedianoNo ratings yet
- Examining The Relationshings Between Parent Experiences and Youth Self-Reports of Slapping-SpankingDocument8 pagesExamining The Relationshings Between Parent Experiences and Youth Self-Reports of Slapping-SpankingCarla Isabel Ramírez SantosNo ratings yet
- Keywords: Risk Behaviour, Violence, Health, Well-Being, Peer Relation, Parent RelationDocument10 pagesKeywords: Risk Behaviour, Violence, Health, Well-Being, Peer Relation, Parent RelationmandaNo ratings yet
- Needs Assessment William Laubach Professor Schedin HSC3713Document5 pagesNeeds Assessment William Laubach Professor Schedin HSC3713api-533734771No ratings yet
- Factors Affecting Bullying Among Junior High Students of Lauis National High SchoolDocument9 pagesFactors Affecting Bullying Among Junior High Students of Lauis National High Schoolcc4684384No ratings yet
- 3B - Group 6 - Reading TextDocument5 pages3B - Group 6 - Reading TextThắm ThắmNo ratings yet
- Research Methods Final Proposal 1Document18 pagesResearch Methods Final Proposal 1api-523816461No ratings yet
- Relationship Status and Obesity RRDocument3 pagesRelationship Status and Obesity RRDon S. VillegasNo ratings yet
- Obesity Research Paper IdeasDocument6 pagesObesity Research Paper Ideasafnhbijlzdufjj100% (1)
- Research Open Access: Suzanne J. Carroll, Theo Niyonsenga, Neil T. Coffee, Anne W. Taylor and Mark DanielDocument16 pagesResearch Open Access: Suzanne J. Carroll, Theo Niyonsenga, Neil T. Coffee, Anne W. Taylor and Mark Danielbrainhub50No ratings yet
- Nutrients 15 04687Document13 pagesNutrients 15 04687Hellen MoreiraNo ratings yet
- How Can Peer Group Influence The Behavior of Adolescents: Explanatory ModelDocument10 pagesHow Can Peer Group Influence The Behavior of Adolescents: Explanatory ModelNISHANTHI EDIRISURIYANo ratings yet
- Final Draft W PaperDocument27 pagesFinal Draft W Paperapi-391688113No ratings yet
- WhoDocument13 pagesWhoKCcheungNo ratings yet
- 003 - Behavioural ScienceDocument8 pages003 - Behavioural ScienceAustin Sams UdehNo ratings yet
- Mental Health in Children and Adolescents With Overweight or ObesityDocument11 pagesMental Health in Children and Adolescents With Overweight or ObesityAnder MathiasNo ratings yet
- Formal 1Document5 pagesFormal 1api-302062745No ratings yet
- The Barriers of Home Environments For Obesity Prevention in Indonesian AdolescentsDocument10 pagesThe Barriers of Home Environments For Obesity Prevention in Indonesian Adolescentsmuammar karimNo ratings yet
- Sexes 03 00002Document20 pagesSexes 03 00002Stella ChanNo ratings yet
- Chapter 1 The Problem and Its Background: Philippines - Statistics & Facts. StatistaDocument37 pagesChapter 1 The Problem and Its Background: Philippines - Statistics & Facts. StatistaKeisha BartolataNo ratings yet
- Social Norms, Contraception and Family Planning: Helpdesk Research ReportDocument15 pagesSocial Norms, Contraception and Family Planning: Helpdesk Research ReportDora ŠtublinNo ratings yet
- Family Process and Peer Influences On Substance Use by AdolescentsDocument18 pagesFamily Process and Peer Influences On Substance Use by AdolescentsRanveer Raj BhatnagarNo ratings yet
- RRLDocument6 pagesRRLmaricar's channelNo ratings yet
- WomenDocument3 pagesWomenamarkumar42012No ratings yet
- Why The Neighborhood Social Environment Is Critical in Obesity PreventionDocument7 pagesWhy The Neighborhood Social Environment Is Critical in Obesity PreventionLink079No ratings yet
- The Impact of Change in Neighborhood Poverty On BMI Trajectory of 37,544 New York City Youth: A Longitudinal StudyDocument11 pagesThe Impact of Change in Neighborhood Poverty On BMI Trajectory of 37,544 New York City Youth: A Longitudinal StudyHitmanNo ratings yet
- Nur340 Eating Disorders and Social MediaDocument8 pagesNur340 Eating Disorders and Social Mediaapi-449016971No ratings yet
- Parental SubstanceDocument17 pagesParental SubstanceeverestchiboliNo ratings yet
- McCabe, M. & Ricciardelli, L. (2003) .Document23 pagesMcCabe, M. & Ricciardelli, L. (2003) .P. NoemiNo ratings yet
- 17874-Article Text-62054-1-10-20230929Document14 pages17874-Article Text-62054-1-10-20230929Sabrina NMNo ratings yet
- Social IsolationDocument10 pagesSocial IsolationBárbara MattosNo ratings yet
- Gender SocializationDocument12 pagesGender SocializationJenjen CabalfinNo ratings yet
- Keluarga 2..12966 - 2016 - Article - 393-1 PDFDocument26 pagesKeluarga 2..12966 - 2016 - Article - 393-1 PDFAisyah GirindraNo ratings yet
- ECOLOGICAL FACTORS AFFECTING CHILDHOOD OBESITY - CHAPTER 1 and CHAPTER 2Document16 pagesECOLOGICAL FACTORS AFFECTING CHILDHOOD OBESITY - CHAPTER 1 and CHAPTER 2Shenna Pitalgo TesoroNo ratings yet
- An20221222 123Document9 pagesAn20221222 123Kainat NasirNo ratings yet
- Up 2Document9 pagesUp 2Sukruth NBNo ratings yet
- Determinants of Diet and Physical Activity in Malaysian Adolescents: A Systematic ReviewDocument28 pagesDeterminants of Diet and Physical Activity in Malaysian Adolescents: A Systematic ReviewonnNo ratings yet
- Marques Et Al 2021 Body Image Accepted ManuscriptDocument41 pagesMarques Et Al 2021 Body Image Accepted ManuscriptYashika Jain -63No ratings yet
- Eng ResearchDocument23 pagesEng ResearchRip GamingNo ratings yet
- Longitudinal Associations Between Parenting Style and Adolescent Disordered Eating BehaviorsDocument8 pagesLongitudinal Associations Between Parenting Style and Adolescent Disordered Eating Behaviorsamm90No ratings yet
- Ruolo Del Comportamento Alimentare Sulla Suscettibilità Genetica All'obesitàDocument10 pagesRuolo Del Comportamento Alimentare Sulla Suscettibilità Genetica All'obesitàTeresa CicconeNo ratings yet
- Parental Monitoring of Adolescents: Current Perspectives for Researchers and PractitionersFrom EverandParental Monitoring of Adolescents: Current Perspectives for Researchers and PractitionersNo ratings yet
- OT Grooming Tooth BrushingDocument3 pagesOT Grooming Tooth BrushingMartha Patricia López PimentelNo ratings yet
- Bonus Printable 8 Myths BustedDocument3 pagesBonus Printable 8 Myths BustedMartha Patricia López PimentelNo ratings yet
- Trying New Foods ChartDocument2 pagesTrying New Foods ChartMartha Patricia López PimentelNo ratings yet
- Autism Medical ComorbiditiesDocument15 pagesAutism Medical ComorbiditiesMartha Patricia López PimentelNo ratings yet
- Intoxicaciones Alimentarias - ConsumidorDocument2 pagesIntoxicaciones Alimentarias - ConsumidorMartha Patricia López PimentelNo ratings yet
- 50 Kid Friendly Meal IdeasDocument2 pages50 Kid Friendly Meal IdeasMartha Patricia López PimentelNo ratings yet
- Parts of Sppech1 PDFDocument42 pagesParts of Sppech1 PDFmshakeel1994No ratings yet
- Identifying PrepositionsDocument2 pagesIdentifying PrepositionsMartha Patricia López PimentelNo ratings yet
- 2 MetabolicDocument8 pages2 MetabolicMartha Patricia López PimentelNo ratings yet
- Representing Knowledge Nonlinguistically - MarzanoDocument3 pagesRepresenting Knowledge Nonlinguistically - MarzanoMartha Patricia López PimentelNo ratings yet
- Medicine Ball WokoutDocument1 pageMedicine Ball WokoutMartha Patricia López PimentelNo ratings yet
- Nutritional Values and Pharmacological Importance of Date Fruit (Phoenix Dactylifera Linn) A ReviewDocument4 pagesNutritional Values and Pharmacological Importance of Date Fruit (Phoenix Dactylifera Linn) A ReviewDr. Md. Shahab UddinNo ratings yet
- Creative Industry R&D Based July 21st 2010Document71 pagesCreative Industry R&D Based July 21st 2010Eng Abdulkadir MahamedNo ratings yet
- Synopsis 313Document13 pagesSynopsis 313yshNo ratings yet
- Euromonitor Said Hrebalife Is #1Document3 pagesEuromonitor Said Hrebalife Is #1tvpaul1958No ratings yet
- Walker Et Al (2009) - The Causes of Porotic Hyperostosis and Cribra Orbitalia A Reappraisal of The Iron Deficiency Anemia Hypothesis. AMERICAN JOURNAL of PHYSICAL ANTHROPOLOGYDocument17 pagesWalker Et Al (2009) - The Causes of Porotic Hyperostosis and Cribra Orbitalia A Reappraisal of The Iron Deficiency Anemia Hypothesis. AMERICAN JOURNAL of PHYSICAL ANTHROPOLOGYPancho ReyesNo ratings yet
- Review of Vegan For Life 2nd EditionDocument3 pagesReview of Vegan For Life 2nd Editiongeorge jacobsNo ratings yet
- Diet ModificationDocument3 pagesDiet ModificationJhayneNo ratings yet
- The Semi Vegan!Document32 pagesThe Semi Vegan!Knut Caspari100% (1)
- Unit 4: Brief History of Aerobics 4.1 Meaning of Aerobics and Dance AerobicsDocument4 pagesUnit 4: Brief History of Aerobics 4.1 Meaning of Aerobics and Dance AerobicsJohn Paul LopezNo ratings yet
- MTHFR Gene Folic Acid and PreventingDocument8 pagesMTHFR Gene Folic Acid and PreventingInez WijayaNo ratings yet
- Unit 4Document12 pagesUnit 4jayswalrameshNo ratings yet
- Horlicks Proffduct ProfileDocument12 pagesHorlicks Proffduct Profileullas2010No ratings yet
- Nursing Theory Case StudyDocument5 pagesNursing Theory Case StudyMuniraNo ratings yet
- Malabsorption SyndromeDocument1 pageMalabsorption SyndromesamanthaNo ratings yet
- FNCP and HTPDocument11 pagesFNCP and HTPJesse SaygoNo ratings yet
- Assessment and Management of Patients With ObesityDocument2 pagesAssessment and Management of Patients With ObesityaliNo ratings yet