You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 8-Hemodynamic Monitoring: Central Venous Pressure (CVP)Document6 pages8-Hemodynamic Monitoring: Central Venous Pressure (CVP)AsmaaYL100% (1)
- REVIEW Cell Adaptation, Injury and DeathDocument101 pagesREVIEW Cell Adaptation, Injury and DeathandiariansyahNo ratings yet
- Relapsing Polychondritis Morphology, Etiology, Pathogenesis and TreatmentDocument1 pageRelapsing Polychondritis Morphology, Etiology, Pathogenesis and TreatmentRiena Austine Leonor NarcillaNo ratings yet
- LESSON PLAN 6 MALARIA IN PREGNANCYjjDocument13 pagesLESSON PLAN 6 MALARIA IN PREGNANCYjjjrkedridgemwanakalandoNo ratings yet
- PPT Inggris DMDocument9 pagesPPT Inggris DMtria WidiastutiNo ratings yet
- Cytokine StormDocument1 pageCytokine StormLNo ratings yet
- Report of Adverse Transfusion Reaction To Blood SuppliersDocument8 pagesReport of Adverse Transfusion Reaction To Blood SuppliersDominic EmerencianaNo ratings yet
- PeriodontitisDocument32 pagesPeriodontitisDimitrios PapadopoulosNo ratings yet
- Ultraformer Flyer Proof PDFDocument2 pagesUltraformer Flyer Proof PDFreception7122No ratings yet
- Medicine MCQS JULY 2023 SOLVEDDocument15 pagesMedicine MCQS JULY 2023 SOLVEDLijo JoNo ratings yet
- Form application for registration of AlbiglutideDocument6 pagesForm application for registration of AlbiglutideMd. Abdur RahmanNo ratings yet
- Headache Clinic CRFDocument12 pagesHeadache Clinic CRFNasirNo ratings yet
- Asuhan Keperawatan Pada Lansia Dengan Gangguan Sistem MuskuloskeletalDocument12 pagesAsuhan Keperawatan Pada Lansia Dengan Gangguan Sistem MuskuloskeletalSiti Nuur Jannah100% (1)
- DR - Ahmed Mowafy - Clinical Book - History & General ExaminationDocument32 pagesDR - Ahmed Mowafy - Clinical Book - History & General ExaminationRancesh FamoNo ratings yet
- T Alimentacion LibroDocument485 pagesT Alimentacion LibrodeadelcarmenNo ratings yet
- ESR Test ExplainedDocument3 pagesESR Test ExplainedbibahNo ratings yet
- Cerebral Palsy Causes and Classification GuideDocument40 pagesCerebral Palsy Causes and Classification Guiderenuka aurangabadkerNo ratings yet
- Solid TumoursDocument48 pagesSolid TumoursViswanadh BNo ratings yet
- Miliaria Types and ManagementDocument4 pagesMiliaria Types and ManagementperpesananNo ratings yet
- APCA Beating - Pain 2nd EdDocument110 pagesAPCA Beating - Pain 2nd EdMichaelNo ratings yet
- PE and HealthDocument3 pagesPE and HealthRia Ellaine Cornelio LachicaNo ratings yet
- NCMB 312 Rle Week 14 Dengue FeverDocument3 pagesNCMB 312 Rle Week 14 Dengue FeverMada mada DaneNo ratings yet
- Final NCP PediaDocument2 pagesFinal NCP PediaKuro HanabusaNo ratings yet
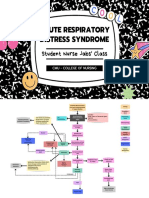
- ARDS Concept Map - BunayogDocument2 pagesARDS Concept Map - BunayogJacela Annsyle BunayogNo ratings yet
- Case StudyDocument5 pagesCase StudyJhosua RoldanNo ratings yet
- Sex Linkage and RecombinationDocument32 pagesSex Linkage and RecombinationRuthie TabanguilNo ratings yet
- Optic Nerve PathologiesDocument64 pagesOptic Nerve Pathologieshasan aslamNo ratings yet
- Renin-Angiotensin-Aldosterone System and CovidDocument10 pagesRenin-Angiotensin-Aldosterone System and CovidnembutalNo ratings yet
- Sunil Prabhudev SonpawaleDocument3 pagesSunil Prabhudev SonpawaleSunil SonpawaleNo ratings yet
- Vol18no8 PDF Version Emerging InfectionsDocument183 pagesVol18no8 PDF Version Emerging InfectionsrehanaNo ratings yet