You might also like
- Congenital Torticollis and Its Physiotherapy Management: Simranjeet KaurDocument8 pagesCongenital Torticollis and Its Physiotherapy Management: Simranjeet KaurEka Wahyu HerdiyantiNo ratings yet
- A Simple Guide to The Posture, Spine Diseases and Use in Disease DiagnosisFrom EverandA Simple Guide to The Posture, Spine Diseases and Use in Disease DiagnosisNo ratings yet
- Christison Lagay2016Document31 pagesChristison Lagay2016Luis Ticona ZegarraNo ratings yet
- Operative Brachial Plexus Surgery: Clinical Evaluation and Management StrategiesFrom EverandOperative Brachial Plexus Surgery: Clinical Evaluation and Management StrategiesAlexander Y. ShinNo ratings yet
- Proceedings: Section ofDocument2 pagesProceedings: Section ofDr LAUMONERIENo ratings yet
- Torticolis-Dr P K SahooDocument4 pagesTorticolis-Dr P K SahooRabiaNo ratings yet
- 7.5 Minor Surgical Conditions of ChildhoodDocument13 pages7.5 Minor Surgical Conditions of ChildhoodΜατθαίος ΠαππάςNo ratings yet
- Torticollis (Wry Neck) : - Hitesh Rohit (3 Year BPT)Document14 pagesTorticollis (Wry Neck) : - Hitesh Rohit (3 Year BPT)Hitesh N RohitNo ratings yet
- Torticollis III BPTDocument31 pagesTorticollis III BPTKASTURI COLLEGENo ratings yet
- Excision of Branchial Cleft CystsDocument10 pagesExcision of Branchial Cleft Cystssjs315No ratings yet
- Flail Chest.Document3 pagesFlail Chest.Irfan ThamrinNo ratings yet
- Kista TiroglosusDocument2 pagesKista TiroglosusKhairuman FitrahNo ratings yet
- Frienchzel Joy A. Asis Group 3 BSN 3-ADocument14 pagesFrienchzel Joy A. Asis Group 3 BSN 3-AKenneth Louis GalizaNo ratings yet
- Coxa SaltansDocument6 pagesCoxa SaltansignashyaNo ratings yet
- Soal Jawaban SpineDocument2 pagesSoal Jawaban Spinepradhanaadhitya100% (1)
- Carlson 2000Document13 pagesCarlson 2000Mamadou DIENENo ratings yet
- Cirugia ToraxDocument117 pagesCirugia ToraxErwin GuerreroNo ratings yet
- Applied Anatomy: Head and NeckDocument9 pagesApplied Anatomy: Head and NeckdivinaNo ratings yet
- Femoral Neck FracturesDocument8 pagesFemoral Neck FracturesMorshed Mahbub AbirNo ratings yet
- Short Papers: Section of OrthopadicsDocument3 pagesShort Papers: Section of OrthopadicscalinNo ratings yet
- Thyroglossal Duct Cyst in Hyoid Bone: Unusual Location: The Journal of Laryngology & OtologyDocument2 pagesThyroglossal Duct Cyst in Hyoid Bone: Unusual Location: The Journal of Laryngology & OtologyTasia RozakiahNo ratings yet
- Jurnal SpondylosisDocument7 pagesJurnal SpondylosisM Hafiz MoulviNo ratings yet
- Diaphyseal Femur FracturesDocument9 pagesDiaphyseal Femur FracturesSoulmates1No ratings yet
- Congenital Muscular TorticolisDocument12 pagesCongenital Muscular TorticolistesfahuntekletilahunNo ratings yet
- Bocca Functional Neck DissectionDocument4 pagesBocca Functional Neck DissectionNoma OlomuNo ratings yet
- Branchial Cleft CystsDocument8 pagesBranchial Cleft CystsHere LeafsNo ratings yet
- Dayyani 2018Document3 pagesDayyani 2018Oswaldo MascareñasNo ratings yet
- Cranio Facial AnomaliDocument60 pagesCranio Facial AnomaliAnne Tjan100% (2)
- Clavicle Fracture: Signs and SymptomsDocument4 pagesClavicle Fracture: Signs and SymptomsbvlbvlNo ratings yet
- Gejala Gangguan JiwaDocument8 pagesGejala Gangguan Jiwakevin stefanoNo ratings yet
- Eagle's Syndrome-15-07-2015 PDFDocument39 pagesEagle's Syndrome-15-07-2015 PDFfahriitoNo ratings yet
- Acquired Torticollis in Children - UpToDateDocument21 pagesAcquired Torticollis in Children - UpToDateZeliha TürksavulNo ratings yet
- Chapter 20: Branchial Cleft Anomalies, Thyroglossal Cysts and Fistulae P. D. M. EllisDocument9 pagesChapter 20: Branchial Cleft Anomalies, Thyroglossal Cysts and Fistulae P. D. M. EllisDrsreeram ValluriNo ratings yet
- Pediatric Orthopaedics: Dr. Zairin Noor Helmi, Spot. (K) .MM - FicsDocument53 pagesPediatric Orthopaedics: Dr. Zairin Noor Helmi, Spot. (K) .MM - FicsmegaFitrianNo ratings yet
- Incidental Reportzaharopoulos2000Document4 pagesIncidental Reportzaharopoulos2000maglangitmarvincNo ratings yet
- Spinal StenosisDocument14 pagesSpinal Stenosisshwampa100% (3)
- Endocranial Lesions in Non-AdultsDocument16 pagesEndocranial Lesions in Non-AdultsAsterios AidonisNo ratings yet
- Cervical Laminectomy: AnatomyDocument9 pagesCervical Laminectomy: AnatomyAgung Choro de ObesNo ratings yet
- Central Neck Dissection For or Recurrent Thyroglossal Duct CystsDocument4 pagesCentral Neck Dissection For or Recurrent Thyroglossal Duct CystsGunduz AgaNo ratings yet
- Fracture FemurDocument28 pagesFracture FemurKulsoom ShahNo ratings yet
- Congenital Talipes Equinovarus 222Document10 pagesCongenital Talipes Equinovarus 222jjjj30No ratings yet
- Double or Bifid Zygomaticus Major Muscle: Anatomy,: Incidence, and Clinical CorrelationDocument4 pagesDouble or Bifid Zygomaticus Major Muscle: Anatomy,: Incidence, and Clinical CorrelationBrijesh MaskeyNo ratings yet
- Orthopedic: Dislocations of The Hip JointDocument16 pagesOrthopedic: Dislocations of The Hip JointAnmarNo ratings yet
- Congenital DysplasiasDocument8 pagesCongenital Dysplasiasyauminnisa hapsariNo ratings yet
- Median (Third) Occipital CondyleDocument4 pagesMedian (Third) Occipital Condylespin_echoNo ratings yet
- Femoral Neck FracturesDocument10 pagesFemoral Neck FracturesMorshed Mahbub AbirNo ratings yet
- Deformities of The SpineDocument112 pagesDeformities of The SpineZunairaNo ratings yet
- Condylar FracturesDocument91 pagesCondylar FracturesSaranya MohanNo ratings yet
- Congenital AbnormalitiesDocument37 pagesCongenital AbnormalitiesrezkadehaNo ratings yet
- C1 (Atlas) FracturesDocument13 pagesC1 (Atlas) FracturesSetyo Budi Premiaji WidodoNo ratings yet
- Examination of The Soft Tissues of The ChestDocument8 pagesExamination of The Soft Tissues of The ChestDum MyNo ratings yet
- Anatomy - Vertebral ColumnDocument5 pagesAnatomy - Vertebral ColumnArmelda Elda MuhollariNo ratings yet
- Ukite 08 AnswersDocument77 pagesUkite 08 AnswersJipin Gopi100% (2)
- Spondylosis Cervical and LumbarDocument9 pagesSpondylosis Cervical and LumbarDr Aamir Yousuf AhangarNo ratings yet
- TRAUMA CuelloDocument17 pagesTRAUMA CuellosantigarayNo ratings yet
- Adcap MedbackDocument15 pagesAdcap MedbackJoanna EdenNo ratings yet
- Electrodiagnosis of Cervical RadiculopathyDocument12 pagesElectrodiagnosis of Cervical RadiculopathywutariNo ratings yet
- Basal Ganglia: Gerhard ReichelDocument8 pagesBasal Ganglia: Gerhard ReichelNelLyNo ratings yet
- Clinical Anatomy of The Knee PDFDocument7 pagesClinical Anatomy of The Knee PDFJuan Victor Briceno OrtizNo ratings yet
- 06 Feb. 2013 Blood - PPT 1Document30 pages06 Feb. 2013 Blood - PPT 1wie_wie_wieNo ratings yet
- Trauma Urogenitalia: DR Marzuki Yusuf Sp.UDocument24 pagesTrauma Urogenitalia: DR Marzuki Yusuf Sp.Uriyadhi_pascaNo ratings yet
- 3.lymphoma Classification UnimalDocument33 pages3.lymphoma Classification Unimalwie_wie_wieNo ratings yet
- TrombusisDocument50 pagesTrombusiswie_wie_wieNo ratings yet
- AnemiaDocument41 pagesAnemiapemburu_gratisNo ratings yet
- Leukemia: Dr. Suhaemi, SPPD, FinasimDocument96 pagesLeukemia: Dr. Suhaemi, SPPD, Finasimwie_wie_wieNo ratings yet
- Mataa JurnalDocument6 pagesMataa JurnalEga Farhatu SuchyarNo ratings yet
- 1.approach To LymphadenopathyDocument54 pages1.approach To LymphadenopathySabila ZathisaNo ratings yet
- Hodgkin's Lymphoma: Rakesh BiswasDocument61 pagesHodgkin's Lymphoma: Rakesh BiswasAsty ModheNo ratings yet
- Mataa JurnalDocument6 pagesMataa JurnalEga Farhatu SuchyarNo ratings yet
- Perdarahan: DR - Suhaemi, SPPD, FinasimDocument27 pagesPerdarahan: DR - Suhaemi, SPPD, Finasimwie_wie_wieNo ratings yet
- Dermatitis KontakDocument13 pagesDermatitis KontakAmanda FairuzNo ratings yet
- 2 NHLDocument13 pages2 NHLwie_wie_wieNo ratings yet
- AnemiaDocument41 pagesAnemiapemburu_gratisNo ratings yet
- Trauma Urogenitalia: DR Marzuki Yusuf Sp.UDocument24 pagesTrauma Urogenitalia: DR Marzuki Yusuf Sp.Uriyadhi_pascaNo ratings yet
- Histology of The Circulatory SystemDocument24 pagesHistology of The Circulatory SystemFatima Zehra YusefNo ratings yet
- KP 6.6 6.7 CardiovascularcorrelatesDocument17 pagesKP 6.6 6.7 Cardiovascularcorrelateswie_wie_wieNo ratings yet
- FSTorticollis JMDocument1 pageFSTorticollis JMRimaTresnawatiNo ratings yet
- Someone Like YouDocument5 pagesSomeone Like Youwie_wie_wieNo ratings yet
- Anemia Defisiensi FeDocument18 pagesAnemia Defisiensi Fewie_wie_wieNo ratings yet
- Limfoma Non HodgkinDocument13 pagesLimfoma Non Hodgkinwie_wie_wieNo ratings yet
- Sample Proposal For GrantDocument8 pagesSample Proposal For GrantRomee SinghNo ratings yet
- Zebra Puzzle GuideDocument3 pagesZebra Puzzle GuideLightFinderNo ratings yet
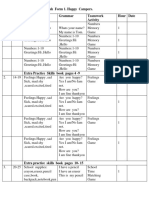
- English Form 1. Happy Campers. Unit Pages Vocabulary Grammar Teamwork Activity Hour DateDocument4 pagesEnglish Form 1. Happy Campers. Unit Pages Vocabulary Grammar Teamwork Activity Hour Dateİlkanə CabbarovaNo ratings yet
- Federación Cinoglosa BelgaDocument2 pagesFederación Cinoglosa Belgalucasl2ossiNo ratings yet
- Radiographic Positioning SummaryDocument10 pagesRadiographic Positioning SummaryCindy100% (1)
- Abdominal Incision1Document11 pagesAbdominal Incision1njoNo ratings yet
- MahitiDocument136 pagesMahitiSandeep RajvamshyNo ratings yet
- African Grey Parrot - WikipediaDocument3 pagesAfrican Grey Parrot - WikipediaWilhelm Richard WagnerNo ratings yet
- Medical Form For NimDocument1 pageMedical Form For NimvishalNo ratings yet
- Walking Movement in RobotDocument24 pagesWalking Movement in RobotNandy ObNo ratings yet
- Hormonal Control ExerciseDocument32 pagesHormonal Control ExerciseamirNo ratings yet
- Anterior Anatomy and The Science of A Natural Smile (OCR)Document146 pagesAnterior Anatomy and The Science of A Natural Smile (OCR)Alfonso Jimenez90% (10)
- Reinforcement and Extension 2Document12 pagesReinforcement and Extension 2Patri Pardellas BlunierNo ratings yet
- Hymns of OrpheusDocument71 pagesHymns of OrpheusJustice DubhghaillNo ratings yet
- Vete 4305 - Group 2 Case Study - Cat With DiabetesDocument19 pagesVete 4305 - Group 2 Case Study - Cat With Diabetesapi-242607157No ratings yet
- Gameshark Pokemon GbaDocument76 pagesGameshark Pokemon Gbanine starNo ratings yet
- TASK SHEET No. 1.2-1 Title: Perform Different Knots Used in Restraining Animals Performance ObjectiveDocument7 pagesTASK SHEET No. 1.2-1 Title: Perform Different Knots Used in Restraining Animals Performance ObjectiveRoh NaldzNo ratings yet
- Lion and Tiger Hybrid: Liger: Presented By: Harsh Salunkhe Xi ScienceDocument14 pagesLion and Tiger Hybrid: Liger: Presented By: Harsh Salunkhe Xi ScienceHarsh SalunkheNo ratings yet
- The 12 Days of ChristmasDocument2 pagesThe 12 Days of ChristmasCarla Muss-JacobsNo ratings yet
- The Tiger in The MenagerieDocument11 pagesThe Tiger in The MenagerieChorch RiderNo ratings yet
- D. L. Bliss State Park HandbookDocument4 pagesD. L. Bliss State Park HandbookCalifornia State ParksNo ratings yet
- BPE109 Module 2.2 Musculoskeletal System PDFDocument7 pagesBPE109 Module 2.2 Musculoskeletal System PDFZedy GullesNo ratings yet
- ĐỀ 48Document7 pagesĐỀ 48bichngocvonagiNo ratings yet
- Bull Terrier Kills ChildDocument1 pageBull Terrier Kills ChildsallyfrankenwarteNo ratings yet
- Toto The Turtle Wid OtherDocument43 pagesToto The Turtle Wid OtherleetolbeanNo ratings yet
- CLS Aipmt-19-20 XI Zoo Study-Package-1 Level-1 Chapter-1 PDFDocument20 pagesCLS Aipmt-19-20 XI Zoo Study-Package-1 Level-1 Chapter-1 PDFJainil PatelNo ratings yet
- Radley Miguel Adarlo - Module 1 Activities Lesson 4-6Document5 pagesRadley Miguel Adarlo - Module 1 Activities Lesson 4-6JK De GuzmanNo ratings yet
- Hematology 1 MidtermsDocument31 pagesHematology 1 Midtermsella SyNo ratings yet
- Basic Spinal KriyaDocument2 pagesBasic Spinal KriyaGabriel C100% (3)
- MadRiverUnion01 27 21editionDocument10 pagesMadRiverUnion01 27 21editionMad River UnionNo ratings yet
- The Obesity Code: Unlocking the Secrets of Weight LossFrom EverandThe Obesity Code: Unlocking the Secrets of Weight LossRating: 4 out of 5 stars4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsFrom EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsNo ratings yet
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeRating: 2 out of 5 stars2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaFrom EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaRating: 4.5 out of 5 stars4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisFrom EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisRating: 4.5 out of 5 stars4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDFrom EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDRating: 5 out of 5 stars5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!From EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Rating: 5 out of 5 stars5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsFrom EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsRating: 5 out of 5 stars5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.From EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Rating: 4.5 out of 5 stars4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerFrom EverandGut: the new and revised Sunday Times bestsellerRating: 4 out of 5 stars4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 4 out of 5 stars4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsFrom EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsRating: 4.5 out of 5 stars4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryFrom EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryRating: 4 out of 5 stars4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessFrom EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessRating: 4.5 out of 5 stars4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisFrom EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisRating: 3.5 out of 5 stars3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningFrom EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningRating: 4 out of 5 stars4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)From EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Rating: 4 out of 5 stars4/5 (378)
- To Explain the World: The Discovery of Modern ScienceFrom EverandTo Explain the World: The Discovery of Modern ScienceRating: 3.5 out of 5 stars3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlFrom EverandThe Marshmallow Test: Mastering Self-ControlRating: 4.5 out of 5 stars4.5/5 (58)