You might also like
- Osgood SlaterDocument5 pagesOsgood Slaterpruebaunodos123No ratings yet
- Bleazey-2012-Recon of Complex Oc Lesions of The Talus With Cylindrical Sponge Allograft and Particulate Juvenile Cartilage GraftDocument7 pagesBleazey-2012-Recon of Complex Oc Lesions of The Talus With Cylindrical Sponge Allograft and Particulate Juvenile Cartilage Graftapi-212907483No ratings yet
- Autogenous Corticocancellous Iliac Bone Graft in Reconstruction of Mandibular Defect: Point of TechniqueDocument4 pagesAutogenous Corticocancellous Iliac Bone Graft in Reconstruction of Mandibular Defect: Point of TechniquekumerrajandrNo ratings yet
- Cuadricepsplastia MipiDocument5 pagesCuadricepsplastia MipiVictor HernandezNo ratings yet
- Marcheggianimuccioli 2019Document12 pagesMarcheggianimuccioli 2019Ghusun MadaniNo ratings yet
- Distal Humeral Fractures-Current Concepts PDFDocument11 pagesDistal Humeral Fractures-Current Concepts PDFRina AlvionitaNo ratings yet
- DR - Sundeep Jeten RajDocument32 pagesDR - Sundeep Jeten Rajselva3333No ratings yet
- A Technical Tip To Treat The Intraoperative Lateral Cortex Fracture During A Medial Open Wedge High Tibial OsteotomyDocument5 pagesA Technical Tip To Treat The Intraoperative Lateral Cortex Fracture During A Medial Open Wedge High Tibial OsteotomyAthenaeum Scientific PublishersNo ratings yet
- Kulkarni2012 PDFDocument7 pagesKulkarni2012 PDFAby SuryaNo ratings yet
- Arthroscopic Synovectomy of The Hip Joint: The Regional Surgical TechniqueDocument7 pagesArthroscopic Synovectomy of The Hip Joint: The Regional Surgical TechniqueMoustafa MohamedNo ratings yet
- Early Outcome After The Use of The Triceps Fascia Flap in Interposition Elbow Arthroplasty A Novel Method in The Treatment of Post-Traumatic Elbow StiffnessDocument6 pagesEarly Outcome After The Use of The Triceps Fascia Flap in Interposition Elbow Arthroplasty A Novel Method in The Treatment of Post-Traumatic Elbow StiffnessJohannes CordeNo ratings yet
- Acl Recon With BPT GraftDocument6 pagesAcl Recon With BPT Graftpaper coe medanNo ratings yet
- Brief Resume of Intended WorkDocument7 pagesBrief Resume of Intended WorkNavin ChandarNo ratings yet
- Fixation of The Distal Tibiofibular Bone-Bridge in Transtibial Amputation PDFDocument4 pagesFixation of The Distal Tibiofibular Bone-Bridge in Transtibial Amputation PDFThomas BowersNo ratings yet
- Outcome Assesment of Proximal Fibular Osteotomy in Medial Compartment Knee OsteoarthritisDocument3 pagesOutcome Assesment of Proximal Fibular Osteotomy in Medial Compartment Knee OsteoarthritisPrashant GuptaNo ratings yet
- All-Epiphyseal, All-Inside Anterior Cruciate Ligament Reconstruction Technique For Skeletally Immature PatientsDocument9 pagesAll-Epiphyseal, All-Inside Anterior Cruciate Ligament Reconstruction Technique For Skeletally Immature Patientshieuminhduong7No ratings yet
- Arthroscopic Fixation of Greater Tuberosity Fractures: A New TechniqueDocument3 pagesArthroscopic Fixation of Greater Tuberosity Fractures: A New Techniqueratnav_ratanNo ratings yet
- Modifying Syme Amputation Prevents Heel Pad MigrationDocument5 pagesModifying Syme Amputation Prevents Heel Pad MigrationdamonenNo ratings yet
- Knupp 2011Document7 pagesKnupp 2011orlandoNo ratings yet
- Reconstruction of The Lateral Tibia Plateau Fracture With A Third Triangular Support Screw: A Biomechanical StudyDocument9 pagesReconstruction of The Lateral Tibia Plateau Fracture With A Third Triangular Support Screw: A Biomechanical StudyNorin FornaNo ratings yet
- Simultaneous Bilateral Opening-Wedge High Tibial Osteotomy With Early Full Weight-Bearing ExerciseDocument8 pagesSimultaneous Bilateral Opening-Wedge High Tibial Osteotomy With Early Full Weight-Bearing Exercisepamelascortez.luanNo ratings yet
- Main. Condromalacia RotulianaDocument4 pagesMain. Condromalacia RotulianaCarmen LaterazaNo ratings yet
- Traatment Gonatroza Prin ArthroplastieDocument5 pagesTraatment Gonatroza Prin Arthroplastieandre_moarcasNo ratings yet
- Journal of Orthopaedic Surgery and ResearchDocument6 pagesJournal of Orthopaedic Surgery and ResearchDewye SartikaNo ratings yet
- Arthroscopic Arthrolysis GuideDocument5 pagesArthroscopic Arthrolysis GuideMoustafa MohamedNo ratings yet
- Total Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDocument4 pagesTotal Knee Arthroplasty in Osteopetrosis Using Patient-Specific InstrumentationDavidBeatonComuladaNo ratings yet
- Alveolar Ridge Augmentation by Distraction OsteogenesisDocument8 pagesAlveolar Ridge Augmentation by Distraction OsteogenesisCarlos Santiago VivenzaNo ratings yet
- Our Experience in Meniscus Tears and Differences in Sport Recovery Between Medial and Lateral Partial Meniscectomy in Young AthleteDocument11 pagesOur Experience in Meniscus Tears and Differences in Sport Recovery Between Medial and Lateral Partial Meniscectomy in Young AthleteAthenaeum Scientific PublishersNo ratings yet
- Surgical Techniques For Complex Proximal Tibial FracturesDocument13 pagesSurgical Techniques For Complex Proximal Tibial FracturesHannah CoNo ratings yet
- 03 de RoeckDocument5 pages03 de RoeckAntonio FagaNo ratings yet
- Arthroscopic Elbow Debridement Using Anterocentral Transbrachialis PortalDocument6 pagesArthroscopic Elbow Debridement Using Anterocentral Transbrachialis PortalMoustafa MohamedNo ratings yet
- Lateral Uka Survivorship Short To MidtermDocument5 pagesLateral Uka Survivorship Short To Midtermapi-267962692No ratings yet
- External Fixation in Trauma of The Foot and AnkleDocument22 pagesExternal Fixation in Trauma of The Foot and AnkleElena ShekaNo ratings yet
- Journal Homepage: - : IntroductionDocument7 pagesJournal Homepage: - : IntroductionIJAR JOURNALNo ratings yet
- Osteoarthritis and Osteoporosis 2Document38 pagesOsteoarthritis and Osteoporosis 2tarikeopsNo ratings yet
- Sliding Bone Graft JournalDocument3 pagesSliding Bone Graft Journalapi-310305222No ratings yet
- Distal Tibia Paper 2Document6 pagesDistal Tibia Paper 2Rajib DebnathNo ratings yet
- Base Segudo Caso ClinicoDocument6 pagesBase Segudo Caso Clinicogatos965669988No ratings yet
- Correction of Malunited Intra-Articular Distal Radius Fractures With An Inside-Out Osteotomy TechniqueDocument6 pagesCorrection of Malunited Intra-Articular Distal Radius Fractures With An Inside-Out Osteotomy TechniqueComunicación PiñalNo ratings yet
- Azar 2003 Otsm Repair of Acute Distal Biceps Tendon RuptureDocument4 pagesAzar 2003 Otsm Repair of Acute Distal Biceps Tendon RuptureKuozram No MasNo ratings yet
- Treatment of Gonarthrosis by Total Knee ArthroplasDocument6 pagesTreatment of Gonarthrosis by Total Knee ArthroplasAhmad MaulanaNo ratings yet
- 4 - Surgical Approaches To The Elbow 2012 Orthopaedics and TraumaDocument6 pages4 - Surgical Approaches To The Elbow 2012 Orthopaedics and TraumaProfesseur Christian DumontierNo ratings yet
- Technique of Reduction and Fixation of Unicondylar Medial Hoffa FracturDocument5 pagesTechnique of Reduction and Fixation of Unicondylar Medial Hoffa Fracturaesculapius100% (1)
- Complications After Arthroscopic Knee SurgeryDocument4 pagesComplications After Arthroscopic Knee SurgeryEma.diazNo ratings yet
- Acl Bone Graft With Mini ArthrotomyDocument9 pagesAcl Bone Graft With Mini Arthrotomypaper coe medanNo ratings yet
- Core Decompression Ankle Pain ReliefDocument9 pagesCore Decompression Ankle Pain ReliefAnonymous kdBDppigENo ratings yet
- Complications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFDocument19 pagesComplications and Outcomes of The Transfibular Approach For Posterolateral Fractures of The Tibial Plateau PDFSergio Tomas Cortés MoralesNo ratings yet
- An Acetabular Fracture With A Series of Complications and Their Solutions A Notable Case ReportDocument6 pagesAn Acetabular Fracture With A Series of Complications and Their Solutions A Notable Case ReportAthenaeum Scientific PublishersNo ratings yet
- 264 2010 Article 1052Document6 pages264 2010 Article 1052thisisangieNo ratings yet
- Schlund 2019Document3 pagesSchlund 2019mesescuNo ratings yet
- Ijrtsat 3 2 6Document4 pagesIjrtsat 3 2 6STATPERSON PUBLISHING CORPORATIONNo ratings yet
- 2021 Treatment of The Temporomandibular Joint Ankylosis With A Customized Prosthesis in A Single Stage The Use of 3D Cutting Guides and Virtual Surgical PlanningDocument4 pages2021 Treatment of The Temporomandibular Joint Ankylosis With A Customized Prosthesis in A Single Stage The Use of 3D Cutting Guides and Virtual Surgical PlanningAlbert OliveraNo ratings yet
- Benech 2013 International Journal of Oral and Maxillofacial SurgeryDocument4 pagesBenech 2013 International Journal of Oral and Maxillofacial SurgerysebitadesantaNo ratings yet
- Boyd Approach To ElbowDocument4 pagesBoyd Approach To ElbowGiulio PriftiNo ratings yet
- A Posterosuperior Approach To The ShoulderDocument5 pagesA Posterosuperior Approach To The ShoulderEllan Giulianno FerreiraNo ratings yet
- Prosthodontic Rehabilitation of A Mandibulectomy Patient - A Clinical ReportDocument4 pagesProsthodontic Rehabilitation of A Mandibulectomy Patient - A Clinical ReportNeha ChughNo ratings yet
- Management of Avn HipDocument13 pagesManagement of Avn Hipterencedsza100% (1)
- Novel Surgical Technique For Clavicle Graft HarvestDocument5 pagesNovel Surgical Technique For Clavicle Graft Harvestsanchaita kohliNo ratings yet
- Tzaveas 2010Document6 pagesTzaveas 2010moonwalker2099No ratings yet
- Cartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesFrom EverandCartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesAaron J. KrychNo ratings yet
- Electric Charge: Conservation and Quantization Conductors, Insulators, and Induced ChargesDocument21 pagesElectric Charge: Conservation and Quantization Conductors, Insulators, and Induced ChargesAcadGucciManeNo ratings yet
- Countable UncountableDocument4 pagesCountable UncountablePaoLo Mena la TorreNo ratings yet
- Astm F477-08Document4 pagesAstm F477-08ALARCONISTANo ratings yet
- The Evolution of Order DiprotodontiaDocument35 pagesThe Evolution of Order DiprotodontiaMarianne Michelle Quiambao de la RosaNo ratings yet
- Energy Monitoring With Ultrasonic Flow MetersDocument35 pagesEnergy Monitoring With Ultrasonic Flow MetersViswa NathanNo ratings yet
- D5293Document8 pagesD5293Carlos Olivares ZegarraNo ratings yet
- Doctors Appointment - 4!14!17 Acid RefluxDocument11 pagesDoctors Appointment - 4!14!17 Acid RefluxRay Edwin Anderson IIINo ratings yet
- 02 - AFT - Know Your Pump & System Curves - Part 2ADocument8 pages02 - AFT - Know Your Pump & System Curves - Part 2AAlfonso José García LagunaNo ratings yet
- Answer Example Source Questio N Type Topic: Glish/Doanddoeshasandhave/Bjgd /post - HTMDocument92 pagesAnswer Example Source Questio N Type Topic: Glish/Doanddoeshasandhave/Bjgd /post - HTMFarhan HakimiNo ratings yet
- Yamaha TT600RE Service ManualDocument382 pagesYamaha TT600RE Service ManualStefan30393% (14)
- Alimak AustraliancontractminingDocument5 pagesAlimak AustraliancontractminingmanudemNo ratings yet
- AIA Design Development Deliverable ListDocument8 pagesAIA Design Development Deliverable Listpeterhwilliams100% (1)
- A Project Report On: "Recreation Club"Document80 pagesA Project Report On: "Recreation Club"Appz100% (2)
- NPTEL Control Engineering Assignment 2 - SEO OptimizedDocument4 pagesNPTEL Control Engineering Assignment 2 - SEO OptimizedGanesh RadharamNo ratings yet
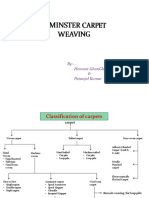
- Axminster CarpetDocument19 pagesAxminster Carpetrohit sinhaNo ratings yet
- 2003 VW Jetta Wiring DiagramsDocument123 pages2003 VW Jetta Wiring DiagramsmikeNo ratings yet
- Coyle Chapter 2 PowerPoint SlidesDocument33 pagesCoyle Chapter 2 PowerPoint SlidesKhaled Sheykh0% (1)
- Discourse on Colonialism and CivilizationDocument48 pagesDiscourse on Colonialism and CivilizationEmir özerNo ratings yet
- STC PDFDocument34 pagesSTC PDFМиша ШаулаNo ratings yet
- BSC Ag Syllabus 5th DeanDocument150 pagesBSC Ag Syllabus 5th Deansaurabh rNo ratings yet
- Wattgate 381 Audio Grade Duplex Socket - y CableDocument20 pagesWattgate 381 Audio Grade Duplex Socket - y Cableapi-11530725100% (1)
- Never Fear, Never Quit - A Story of Courage and Perseverance PDFDocument68 pagesNever Fear, Never Quit - A Story of Courage and Perseverance PDFnaveen100% (2)
- 10 Tips To Protect Yourself From Unhealthy AirDocument2 pages10 Tips To Protect Yourself From Unhealthy AirAnonymous XuFb6TNo ratings yet
- Olympian Generator Brochure 26-200 KvaDocument7 pagesOlympian Generator Brochure 26-200 KvaJawad RazaNo ratings yet
- MSE Admission and Degree RequirementsDocument6 pagesMSE Admission and Degree Requirementsdeathbuddy_87No ratings yet
- Greek MathemaDocument6 pagesGreek MathemaSebastian GhermanNo ratings yet
- EV1116 Manual 146251999-4DDocument32 pagesEV1116 Manual 146251999-4Danitha ferryNo ratings yet
- Diversification in Flavoured Milk: A ReviewDocument6 pagesDiversification in Flavoured Milk: A ReviewInternational Journal of Clinical and Biomedical Research (IJCBR)No ratings yet
- HTP 12 SkodaDocument3 pagesHTP 12 SkodamihnutzuNo ratings yet
- AmadeusDocument3 pagesAmadeusCleofe Mae Piñero AseñasNo ratings yet