You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- PLAB Doable Subject Wise PDFDocument1,645 pagesPLAB Doable Subject Wise PDFAbdiNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 90 TOP THORACIC SURGERY Multiple Choice Questions and Answers PDF 2018Document28 pages90 TOP THORACIC SURGERY Multiple Choice Questions and Answers PDF 2018Ahmed Kassem0% (1)
- Chinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Document11 pagesChinese General Hospital and Medical Center Department of Medical Education and Research Research Ethics Review Board (Rerb)Reda SoNo ratings yet
- CHAPTER 55 - Percutaneous Coronary InterventionDocument1 pageCHAPTER 55 - Percutaneous Coronary InterventionReda SoNo ratings yet
- Ward Reflection PaperDocument1 pageWard Reflection PaperReda SoNo ratings yet
- Answer Key-Mitral ValveDocument6 pagesAnswer Key-Mitral ValveReda SoNo ratings yet
- CH 50 - Approach To Patient With Chest PainDocument1 pageCH 50 - Approach To Patient With Chest PainReda SoNo ratings yet
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoNo ratings yet
- Braunwald Chapter KeypointersDocument6 pagesBraunwald Chapter KeypointersReda SoNo ratings yet
- CHAPTER 27 - Heart Failure With A Preserved Ejection FractionDocument15 pagesCHAPTER 27 - Heart Failure With A Preserved Ejection FractionReda SoNo ratings yet
- Chapter 32 - Genetic Cardiac ArrythmiasDocument7 pagesChapter 32 - Genetic Cardiac ArrythmiasReda SoNo ratings yet
- Name: - Year LevelDocument6 pagesName: - Year LevelReda SoNo ratings yet
- Mitral Valve Disease QuizDocument5 pagesMitral Valve Disease QuizReda SoNo ratings yet
- Private Ward Admission Census 1Document6 pagesPrivate Ward Admission Census 1Reda SoNo ratings yet
- Evidence-Based Approach to Heart Failure History and Physical ExamDocument5 pagesEvidence-Based Approach to Heart Failure History and Physical ExamReda SoNo ratings yet
- Risk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Document7 pagesRisk Factors in Developing Diabetic Foot Ulcers Among Patients in DM Foot Clinic at East Avenue Medical Center From January 2013 To January 2015Reda SoNo ratings yet
- Rapid Response and Cardiac Arrest TeamsDocument11 pagesRapid Response and Cardiac Arrest TeamsReda SoNo ratings yet
- Trials SummaryDocument12 pagesTrials SummaryReda SoNo ratings yet
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Document3 pagesCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoNo ratings yet
- CHAPTER 61: Diabetes and The Cardiovascular System: Ma. Arnee V. Anico-Tondo, M.D., FPCP (CGH)Document1 pageCHAPTER 61: Diabetes and The Cardiovascular System: Ma. Arnee V. Anico-Tondo, M.D., FPCP (CGH)Reda SoNo ratings yet
- Aortic ExamDocument3 pagesAortic ExamReda SoNo ratings yet
- Coronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Document3 pagesCoronary Blood Flow & Myocardial Ischemia Cardiology Fellows Exam July 23, 2018Reda SoNo ratings yet
- 2011 PadDocument19 pages2011 PadReda SoNo ratings yet
- Vascular Conference: JUNE 2018 - MARCH 2019Document2 pagesVascular Conference: JUNE 2018 - MARCH 2019Reda SoNo ratings yet
- Marijuana LegalizationDocument5 pagesMarijuana LegalizationMatt ImpellusoNo ratings yet
- Heart Institute Team Building April 2019Document1 pageHeart Institute Team Building April 2019Reda SoNo ratings yet
- Cardiology census and patient detailsDocument9 pagesCardiology census and patient detailsReda SoNo ratings yet
- Computed Tomography Findings for 8 Cardiovascular PatientsDocument1 pageComputed Tomography Findings for 8 Cardiovascular PatientsReda SoNo ratings yet
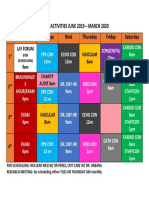
- Daily Activities 2019Document1 pageDaily Activities 2019Reda SoNo ratings yet
- Tilt Table Testing: Name Age/Sex APDocument1 pageTilt Table Testing: Name Age/Sex APReda SoNo ratings yet
- Case Protocol 3Document5 pagesCase Protocol 3Reda SoNo ratings yet
- Case Protocol 3Document2 pagesCase Protocol 3Reda SoNo ratings yet
- Chest Pain in Pediatrics: Tisha K. Yeh, MD and Jay Yeh, MDDocument5 pagesChest Pain in Pediatrics: Tisha K. Yeh, MD and Jay Yeh, MDMahmoud AbouelsoudNo ratings yet
- 312 MR NathanielDocument2 pages312 MR NathanielCarl SantosNo ratings yet
- Cardio NotesDocument7 pagesCardio Notesapi-3744683100% (4)
- Pericardial EffusionDocument41 pagesPericardial Effusionanon_516278156No ratings yet
- Cardiac Tamponad E: Pathophysiology and ManagementDocument105 pagesCardiac Tamponad E: Pathophysiology and ManagementBimaNo ratings yet
- Cvs PBLDocument2 pagesCvs PBLYan RuNo ratings yet
- A Closer Look at Frederic Chopin's Cause of Death PDFDocument2 pagesA Closer Look at Frederic Chopin's Cause of Death PDFRobert SabinNo ratings yet
- Cardiac TamponadeDocument2 pagesCardiac TamponadechoobiNo ratings yet
- Causes and Symptoms of Pericardial EffusionDocument4 pagesCauses and Symptoms of Pericardial EffusionKimberly SolisNo ratings yet
- Nclex ExamDocument18 pagesNclex Examwaqas_xsNo ratings yet
- Clinico Diagnostic Studies On Traumatic Reticulopericarditis in Cattle - A Review of 56 CasesDocument11 pagesClinico Diagnostic Studies On Traumatic Reticulopericarditis in Cattle - A Review of 56 CasesSasikala KaliapanNo ratings yet
- CLOZAPINEDocument14 pagesCLOZAPINEsumaryatiNo ratings yet
- Rheumatic Heart Disease: Infectious Diseases of The HeartDocument5 pagesRheumatic Heart Disease: Infectious Diseases of The HeartVoid LessNo ratings yet
- All of Medicine FlashcardsDocument142 pagesAll of Medicine FlashcardsShaz Chindhy100% (2)
- PericarditisDocument120 pagesPericarditisCalin Popa100% (1)
- AACE Clinical Case ReportsDocument4 pagesAACE Clinical Case ReportsShuaib AhmedNo ratings yet
- Mnemonics On Pathology and MicrobiologyDocument105 pagesMnemonics On Pathology and MicrobiologyJessica Advíncula100% (1)
- Pericarditis and EndocarditisDocument42 pagesPericarditis and Endocarditisicd labNo ratings yet
- Peri, Mio, EndoDocument21 pagesPeri, Mio, Endosalsabilah arrahmanNo ratings yet
- Bates' Guide To Physical Examination and History Taking, 12th EditionDocument12 pagesBates' Guide To Physical Examination and History Taking, 12th EditionmanesNo ratings yet
- Clinchers 100 Important PointsDocument21 pagesClinchers 100 Important PointsNeha GoelNo ratings yet
- Krok!!2023 JanDocument33 pagesKrok!!2023 JanhussainNo ratings yet
- TB Pericarditis Causes and TreatmentDocument14 pagesTB Pericarditis Causes and Treatmentxxxchi chaxxxNo ratings yet
- Tuberculosis Diagnosis and TreatmentDocument46 pagesTuberculosis Diagnosis and TreatmentMoses Jr KazevuNo ratings yet
- Clinical Management of Traumatic Reticuloperitonitis in CattleDocument7 pagesClinical Management of Traumatic Reticuloperitonitis in CattleTaynara BarreiraNo ratings yet
- 12 Lead EKG Interpretation PDFDocument251 pages12 Lead EKG Interpretation PDFRobert So JrNo ratings yet
- Adults 6Document7 pagesAdults 6Bshara SleemNo ratings yet
- Red Flags in Pedia NephrDocument46 pagesRed Flags in Pedia NephrDoaa YoussefNo ratings yet