You might also like
- Direct Deposit FormDocument1 pageDirect Deposit Forms585cvhc22No ratings yet
- Staff Salary FormDocument1 pageStaff Salary FormshafikaNo ratings yet
- Signature Verification FormDocument1 pageSignature Verification FormshahanisubhashNo ratings yet
- Colleague Direct Deposit FormDocument2 pagesColleague Direct Deposit Formtravis stonerNo ratings yet
- Direct Deposit Election FormDocument2 pagesDirect Deposit Election FormAsha Leigh100% (1)
- Paycheck FormDocument1 pagePaycheck Formelanw514No ratings yet
- Consent Letter For Transfer of Funds To Different AccountDocument2 pagesConsent Letter For Transfer of Funds To Different AccountImanNo ratings yet
- wire-transfer-form-18Document1 pagewire-transfer-form-18eghideafesumeNo ratings yet
- Customer Account Activation Request Form: For Individual / Joint Accounts (Non-Resident Customers Only)Document2 pagesCustomer Account Activation Request Form: For Individual / Joint Accounts (Non-Resident Customers Only)Muhammad usman hayatNo ratings yet
- Operating Circular 1 AppendicesDocument6 pagesOperating Circular 1 Appendicespurpel100% (1)
- Direct Dkkfklslndeposit AuthorizationDocument1 pageDirect Dkkfklslndeposit Authorizationpriyansh guptaNo ratings yet
- Ach AngelDocument1 pageAch Angelangel.cavina4No ratings yet
- Account Closure FormatDocument1 pageAccount Closure FormatSaurabh PantNo ratings yet
- Direct Deposit FormDocument1 pageDirect Deposit FormlordpersonNo ratings yet
- Direct Deposit Form 2020 Fill inDocument1 pageDirect Deposit Form 2020 Fill inkfennesseyNo ratings yet
- HOPE YSWP 2023 Bank Verification FormDocument1 pageHOPE YSWP 2023 Bank Verification FormallyNo ratings yet
- Change Coway Payment ModeDocument1 pageChange Coway Payment ModeMonseiur Farhan100% (1)
- Switching Bank Accounts Made EasyDocument5 pagesSwitching Bank Accounts Made EasyTrish HitNo ratings yet
- Axis Bank Customer Request FormDocument2 pagesAxis Bank Customer Request FormAmit Tiwari100% (2)
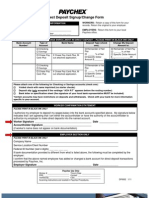
- Direct Deposit Signup FormDocument1 pageDirect Deposit Signup FormMiguel RendonNo ratings yet
- Account Closure FormatDocument2 pagesAccount Closure Formatnibus123No ratings yet
- Axis Travel Currency Card - Refund Form: Transaction DetailsDocument1 pageAxis Travel Currency Card - Refund Form: Transaction Detailsraj_bn4uNo ratings yet
- Alfalah Visa Application FormDocument4 pagesAlfalah Visa Application Formmasoodibrahim100% (1)
- DBapplicationDocument1 pageDBapplicationGM MainstayNo ratings yet
- Customer Request FormDocument2 pagesCustomer Request Formstisspl09No ratings yet
- Application Form StennDocument2 pagesApplication Form StennFrancois Donatien De Sade100% (2)
- Letter of Authorization of PaymentDocument1 pageLetter of Authorization of PaymentJimy Rodolfo Morales CaroNo ratings yet
- Inactive and Dormant Account Activation FormDocument1 pageInactive and Dormant Account Activation Formmani mNo ratings yet
- Account Closure Form - v2Document1 pageAccount Closure Form - v2OTHER Work100% (1)
- How to request a refund from the Civil Service CommissionDocument1 pageHow to request a refund from the Civil Service CommissionIsape Hope Maningo-Burguite Bagaipo100% (1)
- FOREIGN FUNDS TRANSFER REQUEST FORM FOR INDIVIDUALSDocument1 pageFOREIGN FUNDS TRANSFER REQUEST FORM FOR INDIVIDUALSchibykemonday16No ratings yet
- NEFT MandateDocument1 pageNEFT MandateGirishNo ratings yet
- Ofper 4 - Employee Bank Form (Ver. 5 Jul'18)Document1 pageOfper 4 - Employee Bank Form (Ver. 5 Jul'18)okanNo ratings yet
- USCredit ApplicationDocument5 pagesUSCredit ApplicationFSO COMPRESORESNo ratings yet
- Funding Request FormDocument2 pagesFunding Request FormAnne HardeyNo ratings yet
- Fixed / Recurring Deposit Application-Cum-Deposit Slip Date: Deposit Opened in Branch: Branch SOL IDDocument3 pagesFixed / Recurring Deposit Application-Cum-Deposit Slip Date: Deposit Opened in Branch: Branch SOL IDSS56% (16)
- Auto-Offer PSBANKDocument3 pagesAuto-Offer PSBANKAnna KristinaNo ratings yet
- Know Your Customer (KYC) Application FormDocument3 pagesKnow Your Customer (KYC) Application Formbioduny2kNo ratings yet
- New Account Sign Up FormsDocument1 pageNew Account Sign Up FormsMcInnis Enterprises.No ratings yet
- NEFTForm MAX LIFE PDFDocument1 pageNEFTForm MAX LIFE PDFdrantozux100% (1)
- Set up direct deposit with a voided checkDocument1 pageSet up direct deposit with a voided checkNathan SimmonsNo ratings yet
- Withdrawal RequestDocument1 pageWithdrawal RequestGeorge BosnoianNo ratings yet
- Direct Deposit Form 2019Document1 pageDirect Deposit Form 2019Rudolph RushinNo ratings yet
- NewAcctSheet 5.11.22Document2 pagesNewAcctSheet 5.11.22Валера ШаповаловNo ratings yet
- Cash Advance FormDocument1 pageCash Advance FormJann Anthony De-ashes0% (1)
- HLB Cardholder Dispute FormDocument1 pageHLB Cardholder Dispute Formhangtuah79100% (1)
- Direct Deposit FormDocument3 pagesDirect Deposit FormRabindra ShakyaNo ratings yet
- Royal Caribbean Cruises Ltd. Shipboard Seniority Retirement Plan Distribution Election FormDocument2 pagesRoyal Caribbean Cruises Ltd. Shipboard Seniority Retirement Plan Distribution Election FormAldrin Moraes100% (5)
- Order FormDocument1 pageOrder FormGuy RendonNo ratings yet
- Tacoma Capital Application 030719Document2 pagesTacoma Capital Application 030719theodrostadiosNo ratings yet
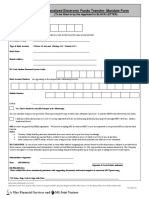
- Nationalized Electronic Funds Transfer-Mandate Form: (To Be Filled in by The Applicant in BLOCK LETTER)Document1 pageNationalized Electronic Funds Transfer-Mandate Form: (To Be Filled in by The Applicant in BLOCK LETTER)Srenu KadariNo ratings yet
- Installment Payment Plan Request: No PO Box NumberDocument4 pagesInstallment Payment Plan Request: No PO Box NumberjackNo ratings yet
- ECS PDF Mandate CitibankDocument8 pagesECS PDF Mandate Citibankbrijesh_chokshi2012No ratings yet
- Paychex Direct Deposit Authorization FormDocument1 pagePaychex Direct Deposit Authorization FormThierry NhamoNo ratings yet
- 4-Direct Deposit InformationDocument1 page4-Direct Deposit InformationqiaoxingliuNo ratings yet
- Credit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!From EverandCredit Report Secrets: How to Understand What Your Credit Report Says About You and What You Can Do About It!Rating: 1 out of 5 stars1/5 (1)
- You’Re a Business Owner, Not a Dummy!: Understand Your Merchant AccountFrom EverandYou’Re a Business Owner, Not a Dummy!: Understand Your Merchant AccountRating: 2 out of 5 stars2/5 (1)
- Ee6461 Eecs Lab Manual 2013 RegulationDocument113 pagesEe6461 Eecs Lab Manual 2013 RegulationshubhNo ratings yet
- Ece 212Document87 pagesEce 212JaneNo ratings yet
- ExpenseDocument1 pageExpenseshubhNo ratings yet
- Wireless CompaniesDocument1 pageWireless CompaniesshubhNo ratings yet
- Ece 212Document87 pagesEce 212JaneNo ratings yet
- 1612 03961Document6 pages1612 03961shubhNo ratings yet
- Ece 212Document87 pagesEce 212JaneNo ratings yet
- Optimal Signature Design For Spread-Spectrum SteganographyDocument15 pagesOptimal Signature Design For Spread-Spectrum SteganographyshubhNo ratings yet
- LocalisedDocument3 pagesLocalisedshubhNo ratings yet
- Outlier Criminall IncidentsDocument16 pagesOutlier Criminall IncidentsshubhNo ratings yet
- RF Direct DepositDocument1 pageRF Direct DepositshubhNo ratings yet
- Application To Candidacy: Expected Conferral Date: February June SeptemberDocument3 pagesApplication To Candidacy: Expected Conferral Date: February June SeptembershubhNo ratings yet
- RF Direct DepositDocument1 pageRF Direct DepositshubhNo ratings yet