You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hi Tracy: Total Due Here's Your Bill For JanuaryDocument6 pagesHi Tracy: Total Due Here's Your Bill For JanuaryalexNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- MMS-TRG-OP-02F3 Narrative ReportDocument14 pagesMMS-TRG-OP-02F3 Narrative ReportCh Ma100% (1)
- Limiting and Excess Reactants Lesson PlanDocument3 pagesLimiting and Excess Reactants Lesson Planapi-316338270100% (3)
- Bluetooth Modules - Martyn Currey PDFDocument64 pagesBluetooth Modules - Martyn Currey PDFAng Tze Wern100% (1)
- B: COVID-19 O: Rief Report Epidemic Trends and Projections in RegonDocument18 pagesB: COVID-19 O: Rief Report Epidemic Trends and Projections in RegonMail TribuneNo ratings yet
- Jackson County Phase 2 Letter of ApprovalDocument1 pageJackson County Phase 2 Letter of ApprovalMail TribuneNo ratings yet
- Jackson County ProclamationDocument2 pagesJackson County ProclamationMail TribuneNo ratings yet
- 2018-19 Oregon School Boards Association Salary Survey BookDocument137 pages2018-19 Oregon School Boards Association Salary Survey BookMail TribuneNo ratings yet
- Roger Stone EndorsementDocument1 pageRoger Stone EndorsementMail TribuneNo ratings yet
- Medford School District Capital Project & Communication AnalysisDocument81 pagesMedford School District Capital Project & Communication AnalysisMail TribuneNo ratings yet
- COVID-19 Intervention Effectiveness and Epidemic Trends For Oregon: A Model-Based AnalysisDocument10 pagesCOVID-19 Intervention Effectiveness and Epidemic Trends For Oregon: A Model-Based AnalysisMail TribuneNo ratings yet
- 2020 06 01 PhaseII Plan Letter FINALDocument12 pages2020 06 01 PhaseII Plan Letter FINALMail TribuneNo ratings yet
- Gov. Kate Brown's Letter - Jackson County Reopening, Phase 1Document1 pageGov. Kate Brown's Letter - Jackson County Reopening, Phase 1Mail TribuneNo ratings yet
- RCC's Design 4 Change MagazineDocument24 pagesRCC's Design 4 Change MagazineMail Tribune100% (1)
- Phoenix-Talent School Board Student Investment Account PresentationDocument14 pagesPhoenix-Talent School Board Student Investment Account PresentationMail TribuneNo ratings yet
- Medford Community OutreachDocument30 pagesMedford Community OutreachMail TribuneNo ratings yet
- Bankruptcy Complaint Prior To Plane CrashDocument8 pagesBankruptcy Complaint Prior To Plane CrashMail TribuneNo ratings yet
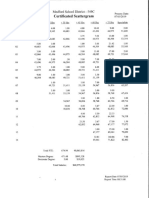
- Medford Teacher Salary ScattergramDocument1 pageMedford Teacher Salary ScattergramMail TribuneNo ratings yet
- 2019-20 Proposed Budget Presentation 042919Document48 pages2019-20 Proposed Budget Presentation 042919Mail TribuneNo ratings yet
- DEQ Jordan Cove Evaluation ReportDocument209 pagesDEQ Jordan Cove Evaluation ReportMail TribuneNo ratings yet
- Subscription Suit Findings of FactDocument127 pagesSubscription Suit Findings of FactMail TribuneNo ratings yet
- DEQ Jordan Cove Evaluation ReportDocument209 pagesDEQ Jordan Cove Evaluation ReportMail TribuneNo ratings yet
- Lawsuit Against Oregon State PoliceDocument27 pagesLawsuit Against Oregon State PoliceMail TribuneNo ratings yet
- Oregon Basin Outlook Report: March 2019Document39 pagesOregon Basin Outlook Report: March 2019Mail TribuneNo ratings yet
- Grand Jury EP Officer Involved ShootingDocument154 pagesGrand Jury EP Officer Involved ShootingMail TribuneNo ratings yet
- Letter To PEA PresidentDocument1 pageLetter To PEA PresidentMail TribuneNo ratings yet
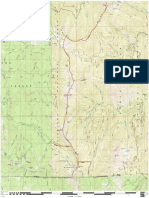
- Boundary National Recreation Trail (RRSNF)Document1 pageBoundary National Recreation Trail (RRSNF)Mail TribuneNo ratings yet
- Prospect Education Association ComplaintDocument4 pagesProspect Education Association ComplaintMail TribuneNo ratings yet
- Transcript of Eagle Point Police Bodycam During Officer-Involved ShootingDocument10 pagesTranscript of Eagle Point Police Bodycam During Officer-Involved ShootingMail TribuneNo ratings yet
- Job Growth Rate Over Time Jackson County (8712)Document1 pageJob Growth Rate Over Time Jackson County (8712)Mail TribuneNo ratings yet
- Graves LawsuitDocument13 pagesGraves LawsuitMail Tribune100% (1)
- District Attorney's Report On Police Shooting in Eagle PointDocument3 pagesDistrict Attorney's Report On Police Shooting in Eagle PointMail Tribune100% (1)
- Boundary National Recreation Trail (Klamath NF)Document1 pageBoundary National Recreation Trail (Klamath NF)Mail TribuneNo ratings yet
- U.S. Tax Court Findings of Fraud On Tax Returns by Curt AnkerbergDocument8 pagesU.S. Tax Court Findings of Fraud On Tax Returns by Curt AnkerbergMail TribuneNo ratings yet
- 4 5895601813654079927 PDFDocument249 pages4 5895601813654079927 PDFqabsNo ratings yet
- Isha Hatha Yoga - Program Registration FormDocument2 pagesIsha Hatha Yoga - Program Registration FormKeyur GadaNo ratings yet
- Checklist For HR Audit Policy and ProceduresDocument3 pagesChecklist For HR Audit Policy and ProcedureskrovvidiprasadaraoNo ratings yet
- Bravo Jr. v. BorjaDocument2 pagesBravo Jr. v. BorjaMaria AnalynNo ratings yet
- BSP Memorandum No. M-2022-035Document1 pageBSP Memorandum No. M-2022-035Gleim Brean EranNo ratings yet
- Operations Management Dr. Loay Salhieh Case Study #1: Students: Hadil Mosa Marah Akroush Mohammad Rajab Ousama SammawiDocument6 pagesOperations Management Dr. Loay Salhieh Case Study #1: Students: Hadil Mosa Marah Akroush Mohammad Rajab Ousama SammawiHadeel Almousa100% (1)
- Introduction To Mass Communication Solved MCQs (Set-3)Document5 pagesIntroduction To Mass Communication Solved MCQs (Set-3)Abdul karim MagsiNo ratings yet
- Soal Ulangan Harian Smester 1 Kelas 8 SMP BAHASA INGGRISDocument59 pagesSoal Ulangan Harian Smester 1 Kelas 8 SMP BAHASA INGGRISsdn6waykhilauNo ratings yet
- Alvin - Goldman - and - Dennis - Whitcomb (Eds) - Social - Epistemology - Essential - Readings - 2011 PDFDocument368 pagesAlvin - Goldman - and - Dennis - Whitcomb (Eds) - Social - Epistemology - Essential - Readings - 2011 PDFOvejaNegra100% (2)
- Drainage Pipe Unit Price AnalysisDocument9 pagesDrainage Pipe Unit Price Analysis朱叶凡No ratings yet
- HSG Anh 9 Thanh Thuy 2 (2018-2019) .Document8 pagesHSG Anh 9 Thanh Thuy 2 (2018-2019) .Huệ MẫnNo ratings yet
- APSEC Summary of Items Discussed in 4/2020 APSEC ForumDocument15 pagesAPSEC Summary of Items Discussed in 4/2020 APSEC Forumyuki michaelNo ratings yet
- Assessment: Bipolar DisorderDocument2 pagesAssessment: Bipolar DisorderMirjana StevanovicNo ratings yet
- Topic 8 - Managing Early Growth of The New VentureDocument11 pagesTopic 8 - Managing Early Growth of The New VentureMohamad Amirul Azry Chow100% (3)
- Impact of Agile On IT and BusinessDocument6 pagesImpact of Agile On IT and BusinessPurva RaneNo ratings yet
- MASM Tutorial PDFDocument10 pagesMASM Tutorial PDFShashankDwivediNo ratings yet
- Module 1: Overview of Implementation of The NSTP (Activities)Document3 pagesModule 1: Overview of Implementation of The NSTP (Activities)RonnelNo ratings yet
- Leaflet STP2025 LightDocument2 pagesLeaflet STP2025 LightNoel AjocNo ratings yet
- Mcquillin Murphy ResumeDocument1 pageMcquillin Murphy Resumeapi-253430225No ratings yet
- Situation AnalysisDocument94 pagesSituation Analysisamirafateha100% (2)
- Resume John BunkerDocument8 pagesResume John BunkerJohn BunkerNo ratings yet
- Talking About Your Home, Furniture and Your Personal Belongings - Third TemDocument4 pagesTalking About Your Home, Furniture and Your Personal Belongings - Third TemTony Cañate100% (1)
- Fact-Sheet Pupils With Asperger SyndromeDocument4 pagesFact-Sheet Pupils With Asperger SyndromeAnonymous Pj6OdjNo ratings yet
- A Story Behind..: Dimas Budi Satria Wibisana Mario Alexander Industrial Engineering 5Document24 pagesA Story Behind..: Dimas Budi Satria Wibisana Mario Alexander Industrial Engineering 5Owais AwanNo ratings yet
- Vol 98364Document397 pagesVol 98364spiveynolaNo ratings yet
- The Conflict With Slavery and Others, Complete, Volume VII, The Works of Whittier: The Conflict With Slavery, Politicsand Reform, The Inner Life and Criticism by Whittier, John Greenleaf, 1807-1892Document180 pagesThe Conflict With Slavery and Others, Complete, Volume VII, The Works of Whittier: The Conflict With Slavery, Politicsand Reform, The Inner Life and Criticism by Whittier, John Greenleaf, 1807-1892Gutenberg.org100% (1)