Professional Documents
Culture Documents
Pediatric Pneumonia
Uploaded by
Krystal Migo Denolo ContrerasCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Pediatric Pneumonia
Uploaded by
Krystal Migo Denolo ContrerasCopyright:
Available Formats
1/11/15
Pediatric Pneumonia
Pediatric Pneumonia
Author: Nicholas John Bennett, MBBCh, PhD, MA(Cantab), FAAP; Chief Editor: Russell W Steele, MD
more...
Updated: Apr 28, 2014
Practice Essentials
The United Nations Children's Fund (UNICEF) estimates that pediatric pneumonia kills 3 million children worldwide
each year. These deaths occur almost exclusively in children with underlying conditions, such as chronic lung
disease of prematurity, congenital heart disease, and immunosuppression. Although most fatalities occur in
developing countries, pneumonia remains a significant cause of morbidity in industrialized nations.
Essential update: Pediatric pneumonia may be effectively treated with twice-daily amoxicillin
In a randomized, placebo-controlled study of 820 pediatric patients with mild pediatric pneumonia, researchers
found that treatment with oral amoxicillin (50 mg/kg/day) twice daily was as effective as amoxicillin given three
times a day. Treatment failure occurred in 23% of the twice-daily group and 22.8% of the thrice-daily group in the
intention-to-treat analysis, and in 21.3% and 20.1% of these groups, respectively, in the per-protocol analysis.
Among the 277 patients with radiologically confirmed pneumonia, treatment failure occurred in 18.8% of patients in
both groups.[1, 2]
Signs and symptoms
Pneumonia can occur at any age, although it is more common in younger children. Pneumonia accounts for 13%
of all infectious illnesses in infants younger than 2 years.
Newborns with pneumonia commonly present with poor feeding and irritability, as well as tachypnea, retractions,
grunting, and hypoxemia. Infections with group B Streptococcus, Listeria monocytogenes, or gram-negative rods
(eg, Escherichia coli, Klebsiella pneumoniae) are common causes of bacterial pneumonia. Group B streptococci
infections are most often transmitted to the fetus in utero. The most commonly isolated virus is respiratory
syncytial virus (RSV).
Cough is the most common symptom of pneumonia in infants, along with tachypnea, retractions, and hypoxemia.
These may be accompanied by congestion, fever, irritability, and decreased feeding. Streptococcus pneumoniae is
by far the most common bacterial pathogen in infants aged 1-3 months.
Adolescents experience similar symptoms to younger children. They may have other constitutional symptoms,
such as headache, pleuritic chest pain, and vague abdominal pain. Vomiting, diarrhea, pharyngitis, and
otalgia/otitis are also common in this age group. Mycoplasma pneumoniae is the most frequent cause of
pneumonia among older children and adolescents.
See Clinical Presentation for more detail.
Diagnosis
The signs and symptoms of pneumonia are often nonspecific and widely vary based on the patients age and the
infectious organisms involved.
Observing the childs respiratory effort during a physical exam is an important first step in diagnosing pneumonia.
The World Health Organization (WHO) respiratory rate thresholds for identifying children with pneumonia are as
follows:
Children younger than 2 months: Greater than or equal to 60 breaths/min
Children aged 2-11 months: Greater than or equal to 50 breaths/min
Children aged 12-59 months: Greater than or equal to 40 breaths/min
Assessment of oxygen saturation by pulse oximetry should be performed early in the evaluation when respiratory
symptoms are present. Cyanosis may be present in severe cases. Capnography may be useful in the evaluation of
children with potential respiratory compromise.
Other diagnostic tests may include the following:
Auscultation by stethoscope
Cultures
Serology
Complete blood cell count (CBC)
Chest radiography
Ultrasonography
New data show that point-of-care ultrasonography accurately diagnoses most cases of pneumonia in children and
young adults. Ultrasonography may eventually replace x-rays for diagnosis.[3, 4]
See Workup for more detail.
emedicine.medscape.com/article/967822-overview
1/12
1/11/15
Pediatric Pneumonia
Management
Initial priorities in children with pneumonia include the identification and treatment of respiratory distress,
hypoxemia, and hypercarbia. Grunting, flaring, severe tachypnea, and retractions should prompt immediate
respiratory support. Children who are in severe respiratory distress should undergo tracheal intubation if they are
unable to maintain oxygenation or have decreasing levels of consciousness. Increased respiratory support
requirements such as increased inhaled oxygen concentration, positive pressure ventilation, or CPAP are
commonly required before recovery begins.
Antibiotics
The majority of children diagnosed with pneumonia in the outpatient setting are treated with oral antibiotics. Highdose amoxicillin is used as a first-line agent for children with uncomplicated community-acquired pneumonia.
Second- or third-generation cephalosporins and macrolide antibiotics such as azithromycin are acceptable
alternatives. Combination therapy (ampicillin and either gentamicin or cefotaxime) is typically used in the initial
treatment of newborns and young infants.
Hospitalized patients can also usually be treated with a narrow-spectrum penicillin such as ampicillin. The choice
of agent and dosing may vary based on local resistance rates (high rates of intermediate or resistant
pneumococcus may require higher dosing of ampicillin to surmount the altered penicillin-binding protein that is the
cause of resistant pneumococcus). In areas where resistance is very high (>25% of strains being nonsusceptible),
a third-generation cephalosporin might be indicated instead. Older children, in addition, may receive a macrolide to
cover for atypical infections.
Although the fluoroquinolones would cover all the common respiratory pathogens of childhood, they are not
approved for this indication and have significant potential adverse effects, including short-term tendon damage and
long-term impact on antibiotic resistance. They should be reserved for cases in which other therapies have failed
and ideally should be used after consultation with an infectious disease specialist with whom other options, or
alternative diagnoses, can be considered.
Children who are toxic appearing should receive antibiotic therapy that includes vancomycin (particularly in areas
where penicillin-resistant pneumococci and methicillin-resistant S aureus [MRSA] are prevalent) along with a
second- or third-generation cephalosporin.
Vaccines
Aside from avoiding infectious contacts (difficult for many families who use daycare facilities), vaccination is the
primary mode of prevention. Influenza vaccine is recommended for children aged 6 months and older. The
pneumococcal conjugate vaccine (PCV13) is recommended for all children younger than 59 months old. The 23valent polysaccharide vaccine (PPVSV) is recommended for children 24 months or older who are at high risk of
pneumococcal disease.
See Treatment and Medication for more detail.
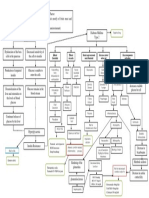
Image library
(Left) Gram stain demonstrating gram-positive cocci in pairs and chains and (right) culture positive for Streptococcus pneumoniae.
Background
Pneumonia and other lower respiratory tract infections are the leading causes of death worldwide. Because
pneumonia is common and is associated with significant morbidity and mortality, properly diagnosing pneumonia,
correctly recognizing any complications or underlying conditions, and appropriately treating patients are important.
Although in developed countries the diagnosis is usually made on the basis of radiographic findings, the World
Health Organization (WHO) has defined pneumonia solely on the basis of clinical findings obtained by visual
inspection and on timing of the respiratory rate. (See Clinical Presentation.)
Pneumonia may originate in the lung or may be a focal complication of a contiguous or systemic inflammatory
process. Abnormalities of airway patency as well as alveolar ventilation and perfusion occur frequently due to
various mechanisms. These derangements often significantly alter gas exchange and dependent cellular
metabolism in the many tissues and organs that determine survival and contribute to quality of life. Recognition,
prevention, and treatment of these problems are major factors in the care of children with pneumonia. (See
Pathophysiology.)
One particular form of pneumonia present in the pediatric population, congenital pneumonia, presents within the
first 24 hours after birth. For more information, see Congenital Pneumonia.
Other respiratory tract diseases such as croup (laryngotracheobronchitis), bronchiolitis, and bronchitis are beyond
the scope of this article and are not discussed further.
Pathophysiology
An inhaled infectious organism must bypass the host's normal nonimmune and immune defense mechanisms in
order to cause pneumonia. The nonimmune mechanisms include aerodynamic filtering of inhaled particles based
on size, shape, and electrostatic charges; the cough reflex; mucociliary clearance; and several secreted
substances (eg, lysozymes, complement, defensins). Macrophages, neutrophils, lymphocytes, and eosinophils
carry out the immune-mediated host defense.
emedicine.medscape.com/article/967822-overview
2/12
1/11/15
Pediatric Pneumonia
Respiratory tract host defenses
To prevent and minimize injury and invasion by microorganisms and foreign substances, various defense
mechanisms have evolved, both systemically and within the respiratory tract. Some mechanisms are nonspecific
and are directed against any invasive agent, whereas others are targeted against only microbes or substances
with specific antigenic determinants. Many of the defenses are compromised in the fetus and newborn infant,
resulting in more frequent breaches and consequent disruption of normal lung structure and function.[5]
Nonspecific defenses include the glottis and vocal cords, ciliary escalator, airway secretions, migratory and fixed
phagocytes, nonspecific antimicrobial proteins and opsonins, and the normal relatively nonpathogenic airway flora.
Anatomic structures of the upper airway and associated reflexes discourage particulate material from entering,
whereas coordinated movement of the microscopic cilia on the tracheal and bronchial epithelia tends to sweep
particles and mucus up the airway and away from the alveoli and distal respiratory structures.
Mucoid airway secretions provide a physical barrier that minimizes epithelial adhesion and subsequent invasion by
microorganisms. These secretions typically contain complement components, fibronectin, and other proteins that
bind to microbes and render them more susceptible to ingestion by phagocytes. Alveolar and distal airway
secretions also include whole surfactant, which facilitates opsonization and phagocytosis of pathogens, as well as
surfactant-associated proteins A (Sp-A) and D (Sp-D), both of which modulate phagocytosis, phagocyte
production of oxyradicals, and cytokine elaboration.
The secretions also contain directly inhibitory and microbicidal agents, such as iron-binding proteins, lysozymes,
and defensins. Typical benign airway commensals, such as alpha-hemolytic streptococci and coagulase-negative
staphylococci, occupy mucosal sites and elaborate bacteriocins and other substances that prevent more
pathogenic organisms from adhesion, replication, and possible opportunistic invasion.
Newborns typically have sterile respiratory mucosa at birth, with subsequent uncontested colonization by
microorganisms from the mother or environment. Accelerated access to distal respiratory structures and bypass of
much of the ciliary escalator occur in infants who require endotracheal intubation. In these infants, increased
physical disruption of epithelial and mucous barriers also occurs. In addition, interventional exposure to high
oxygen concentrations, generous airway pressures, and large intrapulmonary gas volumes may interfere with
ciliary function and mucosal integrity. The use of less invasive means of respiratory support, such as nasal
ventilation, nasal continuous positive airway pressure (CPAP), and nasal cannula (conventional or humidified, high
flow), may produce lesser degrees of pulmonary mucosal and parenchymal disruption, but some disruption is
almost always present.
Systemic host defenses
Immunologic defense mechanisms targeted against particular pathogens typically emanate from specifically
primed lymphocytes following presentation of processed antigens by macrophages. These mechanisms include
cytotoxic, killer, suppressor, and memory functions; systemic and secretory antibodies; and consequent
cascades of cytokines, complement, vasomotor regulatory molecules, hemostatic factors, and other agents.
Secretory antibodies are typically multimeric and contain secretory component and J chains that render them
more opsonic and more resistant to microbial proteases.
Many of the biochemical cascades triggered by specific immune responses serve to localize microbial invasion,
amplify and focus recruitment of phagocytes to the affected sites, and directly disrupt the structural and metabolic
integrity of the microbes. The role that these cascades play in triggering apoptosis (programmed cell death) in
host and invader cells is still undergoing exploration.
Secretory antibodies and mucosal lymphoid tissue are absent or minimally functional for the first month of life
postnatally. Systemic antibodies may enter pulmonary tissues but usually consist primarily of passively
transmitted maternal antibodies, with reduced transplacental transport of maternal antibodies before 32 weeks'
gestation. Specific systemic antibodies can be generated, but many components of the necessary immunologic
machinery are relatively sluggish. Circulating complement components are present at approximately 50% of the
concentration found in older children, although components of the alternative pathway are present in sufficient
quantities to serve as effective opsonins.
The neonatal granulocyte number frequently decreases in response to early infection (as well as noninflammatory
processes such as maternal preeclampsia), whereas the phagocytes that are present often move much more
sluggishly to the inflammatory focus, whether it is a microorganism or inanimate debris. Once at the targeted
sites, phagocytes often ingest the invaders less efficiently, although intracellular microbicidal activities appear
normal. Intercellular communication via cytokines and other mediators is blunted.
The net result of these and other developmental aberrations is that the fetal and neonatal inflammatory response is
slower, less efficient, and much less focused than in older children. Infection is less likely to be localized and
effectively inhibited by host defenses alone. Inflammation from particulate debris and other foreign substances is
isolated less effectively, and the injurious effector portions of the inflammatory cascade are much less precisely
targeted.
Pathogenesis
Pneumonia is characterized by inflammation of the alveoli and terminal airspaces in response to invasion by an
infectious agent introduced into the lungs through hematogenous spread or inhalation. The inflammatory cascade
triggers the leakage of plasma and the loss of surfactant, resulting in air loss and consolidation.
The activated inflammatory response often results in targeted migration of phagocytes, with the release of toxic
substances from granules and other microbicidal packages and the initiation of poorly regulated cascades (eg,
complement, coagulation, cytokines). These cascades may directly injure host tissues and adversely alter
endothelial and epithelial integrity, vasomotor tone, intravascular hemostasis, and the activation state of fixed and
migratory phagocytes at the inflammatory focus. The role of apoptosis (noninflammatory programmed cell death) in
pneumonia is poorly understood.
emedicine.medscape.com/article/967822-overview
3/12
1/11/15
Pediatric Pneumonia
Pulmonary injuries are caused directly and/or indirectly by invading microorganisms or foreign material and by
poorly targeted or inappropriate responses by the host defense system that may damage healthy host tissues as
badly or worse than the invading agent. Direct injury by the invading agent usually results from synthesis and
secretion of microbial enzymes, proteins, toxic lipids, and toxins that disrupt host cell membranes, metabolic
machinery, and the extracellular matrix that usually inhibits microbial migration.
Indirect injury is mediated by structural or secreted molecules, such as endotoxin, leukocidin, and toxic shock
syndrome toxin-1 (TSST-1), which may alter local vasomotor tone and integrity, change the characteristics of the
tissue perfusate, and generally interfere with the delivery of oxygen and nutrients and removal of waste products
from local tissues.[6, 7]
On a macroscopic level, the invading agents and the host defenses both tend to increase airway smooth muscle
tone and resistance, mucus secretion, and the presence of inflammatory cells and debris in these secretions.
These materials may further increase airway resistance and obstruct the airways, partially or totally, causing
airtrapping, atelectasis, and ventilatory dead space. In addition, disruption of endothelial and alveolar epithelial
integrity may allow surfactant to be inactivated by proteinaceous exudate, a process that may be exacerbated
further by the direct effects of meconium or pathogenic microorganisms.
In the end, conducting airways offer much more resistance and may become obstructed, alveoli may be atelectatic
or hyperexpanded, alveolar perfusion may be markedly altered, and multiple tissues and cell populations in the
lung and elsewhere sustain injury that increases the basal requirements for oxygen uptake and excretory gas
removal at a time when the lungs are less able to accomplish these tasks.
Alveolar diffusion barriers may increase, intrapulmonary shunts may worsen, and ventilation/perfusion (V/Q)
mismatch may further impair gas exchange despite endogenous homeostatic attempts to improve matching by
regional airway and vascular constriction or dilatation. Because the myocardium has to work harder to overcome
the alterations in pulmonary vascular resistance that accompany the above changes of pneumonia, the lungs may
be less able to add oxygen and remove carbon dioxide from mixed venous blood for delivery to end organs. The
spread of infection or inflammatory response, either systemically or to other focal sites, further exacerbates the
situation.
Viral infections are characterized by the accumulation of mononuclear cells in the submucosa and perivascular
space, resulting in partial obstruction of the airway. Patients with these infections present with wheezing and
crackles (see Clinical Presentation). Disease progresses when the alveolar type II cells lose their structural
integrity and surfactant production is diminished, a hyaline membrane forms, and pulmonary edema develops.
In bacterial infections, the alveoli fill with proteinaceous fluid, which triggers a brisk influx of red blood cells (RBCs)
and polymorphonuclear (PMN) cells (red hepatization) followed by the deposition of fibrin and the degradation of
inflammatory cells (gray hepatization). During resolution, intra-alveolar debris is ingested and removed by the
alveolar macrophages. This consolidation leads to decreased air entry and dullness to percussion; inflammation in
the small airways leads to crackles (see Clinical Presentation).
Four stages of lobar pneumonia have been described. In the first stage, which occurs within 24 hours of infection,
the lung is characterized microscopically by vascular congestion and alveolar edema. Many bacteria and few
neutrophils are present. The stage of red hepatization (2-3 d), so called because of its similarity to the consistency
of liver, is characterized by the presence of many erythrocytes, neutrophils, desquamated epithelial cells, and
fibrin within the alveoli. In the stage of gray hepatization (2-3 d), the lung is gray-brown to yellow because of
fibrinopurulent exudate, disintegration of RBCs, and hemosiderin. The final stage of resolution is characterized by
resorption and restoration of the pulmonary architecture. Fibrinous inflammation may lead to resolution or to
organization and pleural adhesions.
Bronchopneumonia, a patchy consolidation involving one or more lobes, usually involves the dependent lung
zones, a pattern attributable to aspiration of oropharyngeal contents. The neutrophilic exudate is centered in
bronchi and bronchioles, with centrifugal spread to the adjacent alveoli.
In interstitial pneumonia, patchy or diffuse inflammation involving the interstitium is characterized by infiltration of
lymphocytes and macrophages. The alveoli do not contain a significant exudate, but protein-rich hyaline
membranes similar to those found in adult respiratory distress syndrome (ARDS) may line the alveolar spaces.
Bacterial superinfection of viral pneumonia can also produce a mixed pattern of interstitial and alveolar airspace
inflammation.
Miliary pneumonia is a term applied to multiple, discrete lesions resulting from the spread of the pathogen to the
lungs via the bloodstream. The varying degrees of immunocompromise in miliary tuberculosis (TB),
histoplasmosis, and coccidioidomycosis may manifest as granulomas with caseous necrosis to foci of necrosis.
Miliary herpesvirus, cytomegalovirus (CMV), or varicella-zoster virus infection in severely immunocompromised
patients results in numerous acute necrotizing hemorrhagic lesions.
Etiology
Pneumonia can be caused by a myriad of microorganisms. Clinical suspicion of a particular offending agent is
derived from clues obtained during the history and physical examination. While virtually any microorganism can
lead to pneumonia, specific bacterial, viral, fungal, and mycobacterial infections are most common in previously
healthy children. The age of infection, exposure history, risk factors for unusual pathogens, and immunization
history all provide clues to the infecting agent.
In a prospective multicenter study of 154 hospitalized children with acute community-acquired pneumonia (CAP) in
whom a comprehensive search for an etiology was sought, a pathogen was identified in 79% of children. Pyogenic
bacteria accounted for 60% of cases, of which 73% were due to Streptococcus pneumoniae, while the atypical
bacteria Mycoplasma pneumoniae and Chlamydophila pneumoniae were detected in 14% and 9%, respectively.
Viruses were documented in 45% of children. Notably, 23% of the children had concurrent acute viral and bacterial
disease. In the study, preschool-aged children had as many episodes of atypical bacterial lower respiratory
infections as older children. Multivariable analyses revealed that high temperature (38.4C) within 72 hours after
admission and the presence of pleural effusion were significantly associated with bacterial pneumonia.[8]
emedicine.medscape.com/article/967822-overview
4/12
1/11/15
Pediatric Pneumonia
Specific etiologic agents vary based on age groups (ie, newborns, young infants, infants and toddlers, 5-year-olds,
school-aged children and young adolescents, older adolescents).
Newborns
In newborns (age 0-30 d), organisms responsible for infectious pneumonia typically mirror those responsible for
early onset neonatal sepsis. This is not surprising in view of the role that maternal genitourinary and
gastrointestinal tract flora play in both processes. Infections with group B Streptococcus, Listeria monocytogenes,
or gram-negative rods (eg, Escherichia coli, Klebsiella pneumoniae) are common causes of bacterial pneumonia.
These pathogens can be acquired in utero, via aspiration of organisms present in the birth canal, or by postnatal
contact with other people or contaminated equipment.
Group B Streptococcus (GBS) was the most common bacterial isolate in most locales from the late 1960s to the
late 1990s, when the impact of intrapartum chemoprophylaxis in reducing neonatal and maternal infection by this
organism became evident. E coli has become the most common bacterial isolate among VLBW infants (1500 g or
less) since that time.[9] Other potential bacterial organisms include the following:
Nontypeable Haemophilus influenzae (NTHi)
Other gram-negative bacilli
Enterococci
Staphylococcus aureus
Some organisms acquired perinatally may not cause illness until later in infancy, including Chlamydia trachomatis,
U urealyticum, Mycoplasma hominis, CMV, and Pneumocystis carinii. C trachomatis organisms are presumably
transmitted at birth during passage through an infected birth canal, although most infants are asymptomatic during
the first 24 hours and develop pneumonia only after the first 2 weeks of life.
Group B streptococci infections are most often transmitted to the fetus in utero, usually as a result of colonization
of the mother's vagina and cervix by the organism. Agents of chronic congenital infection, such as CMV,
Treponema pallidum (the cause of pneumonia alba), Toxoplasma gondii, and others, may cause pneumonia in the
first 24 hours of life. The clinical presentation usually involves other organ systems as well.
Community-acquired viral infections occur in newborns, although less commonly than in older infants. The most
commonly isolated virus is respiratory syncytial virus (RSV). The transfer of maternal antibodies is important in
protecting newborns and young infants from such infections, making premature infants (who may not have
benefited from sufficient transfer of transplacental immunoglobulin [Ig] G]) especially vulnerable to lower-tract
disease. In addition, premature infants may have chronic lung disease of prematurity, with associated
hyperreactive airways, fewer functional alveoli, and baseline increased oxygen requirements.
Newborns may also be affected by the bacteria and viruses that commonly cause infections in older infants and
children. Risk factors for infection include older siblings, group daycare, and lack of immunization.
Young infants
In the young infant (aged 1-3 mo), continued concern about the perinatally acquired pathogens mentioned above
remains. However, most bacterial pneumonia in this age group is community acquired and involves S pneumoniae,
S aureus, and nontypeable H influenzae. S pneumoniae is by far the most common bacterial pathogen in this age
group. Infection with any of these pyogenic bacteria may be complicated by lung abscess, parapneumonic
effusions, and empyema, although S aureus is notorious for such complications.[10]
At this age, infants are incompletely immunized and remain at higher risk for H influenzae type B and
pneumococcal disease, although herd immunity gained from widespread immunization of the population has been
broadly protective. It is important to note that the current conjugate pneumococcal vaccine provides protection
against 13 common pneumococcal types, but nonvaccine types remain problematic.
Most lower respiratory tract disease in young infants occurs during the respiratory virus season and is viral in
origin, particularly in the patient with clinical bronchiolitis. The most common viral agents include RSV,
parainfluenza viruses, influenza virus, adenovirus, and human metapneumovirus (hMPV).
Atypical organisms may rarely cause infection in infants. Of these, C trachomatis, U urealyticum, CMV, and P
carinii are described.
Bordetella pertussis infection leads to pneumonia in as many as 20% of infected infants (as a complication of the
whooping cough infection).
Among other potential atypical bacterial pathogens, U urealyticum and U parvum have been recovered from
endotracheal aspirates shortly after birth in very low birth weight (VLBW) infants and have been variably associated
with various adverse pulmonary outcomes, including bronchopulmonary dysplasia (BPD).[11, 12, 13, 14] Whether
these organisms are causal or simply a marker of increased risk is unclear.
Infants, toddlers, and preschool-aged children
Viruses remain the most common cause of pneumonia in this age group, accounting for approximately 90% of all
lower respiratory tract infections. Tsolia et al identified a viral infection among 65% of hospitalized children with
community-acquired pneumonia.[15]
RSV is the most common viral pathogen, followed by parainfluenza types 1, 2, and 3 and influenza A or B. RSV
infection occurs in the winter and early spring. Parainfluenza type 3 infection occurs in the spring, and types 1 and
2 occur in the fall. Influenza occurs in the winter.
Other viruses that cause pneumonia less frequently in infants and young children include adenovirus, enterovirus,
rhinovirus, and coronavirus. A recent addition to this list is hMPV, which causes an illness similar to RSV and
may be responsible for one third to one half of non-RSV bronchiolitis. The herpesviruses (HSV, VZV, and CMV)
emedicine.medscape.com/article/967822-overview
5/12
1/11/15
Pediatric Pneumonia
may rarely cause pneumonia, particularly in children with impaired immune systems.
Bacterial infections in this age group are seen on a regular basis. S pneumoniae is by far the most common
bacterial cause of pneumonia. Among hospitalized children with bacterial pneumonia, S pneumoniae accounts for
21-44% of disease.[8, 16, 17] Other agents to consider include H influenzae type B (HiB) (very uncommon in
immunized children[18] ), S pyogenes, and S aureus.
Children younger than 5 years, children enrolled in daycare, or those with frequent ear infections are at increased
risk for invasive pneumococcal disease and infection with resistant pneumococcal strains. Evidence suggests that
breastfeeding has a protective effect against invasive pneumococcal infection.
School-aged children and young adolescents
M pneumoniae is the most frequent cause of pneumonia among older children and adolescents. Mycoplasma
accounts for 14-35% of pneumonia hospitalizations in this age group.[8, 15, 19] Children in homeless shelters and
group homes and those with household contacts are at particular risk. Similarly, the diagnosis must be considered
in immunocompromised children.
In this age group, pyogenic bacterial pneumonia remains a concern, usually caused by S pneumoniae. Other
pyogenic bacterial pathogens to consider include S aureus and S pyogenes.
Chlamydophila pneumoniae also causes pneumonia. The related organism, C psittaci, is an unusual cause of
pneumonia that occurs in people who work with and handle birds.
In immunosuppressed individuals, opportunistic infections with organisms such as Aspergillus species,
Pneumocystis jirovecii, and CMV can occur.
Viral pneumonia remains common in this age group. Influenza pneumonia is a particular concern because ongoing
infection with this virus predisposes to the development of bacterial superinfection, usually with S pneumoniae or S
aureus.
Older adolescents
M pneumoniae is the most common cause of community-acquired pneumonia during the teenage and young adult
years. Atypical pneumonia caused by C pneumoniae can present with identical signs and symptoms. Bacterial
pneumonia caused by S pneumoniae is also seen.
Pulmonary infections caused by dimorphic fungi are also seen in this age group. Histoplasma capsulatum, which
is found in nitrate-rich soil, is usually acquired as a result of inhalation of spores. Chicken coops and other bird
roosts and decaying wood are often-cited sources. Cryptococcus neoformans is a common infection among
pigeon breeders, but it is unusual in other immunocompetent individuals.
Blastomyces dermatitides, another dimorphic fungus, is found in certain geographic locations, most notably the
Ohio and Mississippi River valleys. As with histoplasmosis, blastomycosis is acquired by inhalation of spores.
Although 3 distinct forms of infection exist, the most common is acute pneumonia, which, in previously healthy
individuals, most often resolves without treatment.
Viral pneumonias are common in this age group are usually mild and self-limited, but influenza pneumonia can be
severe or protracted, particularly when a bacterial infection follows.
TB pneumonia in children warrants special mention. It can occur in any age group, and it is important to remember
that children with TB usually do not present with symptoms until 1-6 months after primary infection. Any child with
pneumonia who has a history of TB exposure, or who has traveled to a TB-endemic area of the world needs to be
fully evaluated for the possibility of tuberculosis.
Legionella pneumophila, the agent of Legionnaires disease, can also cause pneumonia, although it is uncommon
in the pediatric age group.
Not all pneumonia is caused by infectious agents. Children who have severe gastroesophageal reflux (GERD) may
develop chemical pneumonitis secondary to recurrent aspiration. Inhalation of certain chemicals or smoke may
cause pulmonary inflammation. Additionally, aspiration pneumonia is more common in children with neurologic
impairment, swallowing abnormalities, gastrointestinal motility, or a gastrostomy tube. Oral anaerobic flora, with or
without aerobes, is the most common etiologic agent.
Immunocompromised children
Some children who are immunocompromised, whether secondary to HIV infection/AIDS, an immune disorder, or
chemotherapy for a malignancy, are at risk for pneumonias with opportunistic agents. Virtually any bacteria, virus,
fungus, or even parasite can invade and infect the lungs if the immune system is sufficiently impaired. Carefully
obtained samples for appropriate microbiologic testing are paramount in such patients so that therapy can be
optimized.
Children with cystic fibrosis are especially prone to develop infections with S aureus, Pseudomonas aeruginosa,
Burkholderia cepacia, and other multidrug-resistant organisms.
P jirovecii pneumonia (PCP) is common in the most severely compromised children and can lead to respiratory
failure and death in those who are profoundly immunocompromised. Adenovirus infections can be severe in these
children as well, leading to bronchiolitis obliterans or hyperlucent lung syndrome. In addition, CMV poses a great
risk to immunocompromised patients.
Fungal pneumonia, caused by Aspergillus, Zygomycetes, or other related fungi, occur in immunocompromised
patients who undergo prolonged hospitalization, have prolonged neutropenia, and/or have received broad-spectrum
antibiotics. Patients with underlying hematologic malignancies are at the highest risk.
emedicine.medscape.com/article/967822-overview
6/12
1/11/15
Pediatric Pneumonia
Patients with sickle cell disease have problems with their complement system as well as functional asplenia,
which predisposes them to infection with encapsulated organisms such as S pneumoniae and H influenzae type
B. M pneumoniae is also a common agent of pneumonia is this group of patients.
Epidemiology
United States statistics
Pneumonia can occur at any age, although it is more common in younger children. Pneumonia accounts for 13%
of all infectious illnesses in infants younger than 2 years. In a large community-based study conducted by Denny
and Clyde, the annual incidence rate of pneumonia was 4 cases per 100 children in the preschool-aged group, 2
cases per 100 children aged 5-9 years, and 1 case per 100 children aged 9-15 years.[20]
Thompson et al reported that, after elderly persons, the second highest rates of influenza-associated
hospitalizations in the United States were in children younger than 5 years.[21] The investigators evaluated annual
influenza-associated hospitalizations by hospital discharge category, discharge type, and age group.
In a randomized double-blind trial, the heptavalent pneumococcal vaccine reduced the incidence of clinically
diagnosed and radiographically diagnosed pneumonia among children younger than 5 years by 4% and 20%,
respectively.[22] Although the overall rate of pneumonia has decreased in the United States with the use of the 7valent vaccine, the rate of empyema and complicated pneumonia has increased.[23] With the use of the 13-valent
conjugated pneumococcal polysaccharide vaccine, the overall rates of pneumonia are anticipated to drop further.
The new vaccine includes serotypes that have become associated with complicated or antibiotic-resistant disease
(19A and 6A, for example).
In school-aged children and adolescents, bronchopneumonia occurs in 0.8-2% of all pertussis cases and 16-20%
of hospitalized cases. M pneumoniae accounts for 14-35% of pneumonia hospitalizations in this age group,[8, 15,
19]
and mycobacterial pneumonia has recently been noted with increasing frequency in some inner-city areas,
particularly children in homeless shelters and group homes and those with household contacts.
International statistics
Pneumonia and other lower respiratory tract infections are the leading cause of death worldwide. The WHO Child
Health Epidemiology Reference Group estimated the median global incidence of clinical pneumonia to be 0.28
episodes per child-year.[24] This equates to an annual incidence of 150.7 million new cases, of which 11-20 million
(7-13%) are severe enough to require hospital admission. Ninety-five percent of all episodes of clinical pneumonia
in young children worldwide occur in developing countries.
Approximately 150 million new cases of pneumonia occur annually among children younger than 5 years
worldwide, accounting for approximately 10-20 million hospitalizations.[20] A WHO Child Health Epidemiology
Reference Group publication cited the incidence of community-acquired pneumonia among children younger than 5
years in developed countries as approximately 0.026 episodes per child-year,[24] and a study conducted in the
United Kingdom showed that 59% of deaths from pertussis are associated with pneumonia.
Prognosis
Overall, the prognosis is good. Most cases of viral pneumonia resolve without treatment; common bacterial
pathogens and atypical organisms respond to antimicrobial therapy (see Treatment and Management). Long-term
alteration of pulmonary function is rare, even in children with pneumonia that has been complicated by empyema
or lung abscess.
Patients placed on a protocol-driven pneumonia clinical pathway are more likely to have favorable outcomes. The
prognosis for varicella pneumonia is somewhat more guarded. Staphylococcal pneumonia, although rare, can be
very serious despite treatment.
Morbidity
Although viral pneumonias are common in school-aged children and adolescents and are usually mild and selflimited, these pneumonias are occasionally severe and can rapidly progress to respiratory failure, either as a
primary manifestation of viral infection or as a consequence of subsequent bacterial infection.
Morbidity and mortality from RSV and other viral infections is higher among premature infants and infants with
underlying lung disease. Significant sequelae occur with adenoviral disease, including bronchiolitis obliterans and
necrotizing bronchiolitis. With neonatal pneumonia, even if the infection is eradicated, many hosts develop longlasting or permanent pulmonary changes that affect lung function, the quality of life, and susceptibility to later
infections.
Infants and postpubertal adolescents with TB pneumonia are at increased risk of disease progression. If TB is not
treated during the early stages of infection, approximately 25% of children younger than 15 years develop
extrapulmonary disease.
Bronchopneumonia occurs in 0.8-2% of all pertussis cases and 16-20% of hospitalized cases; the survival rate of
these patients is much lower than in those with pneumonia that is attributed to other causes.
Immunocompromised children, those with underlying lung disease, and neonates are at high risk for severe
sequelae, and they are also susceptible to various comorbidities. Cryptococcosis may occur in as many as 5-10%
of patients with AIDS, and acute chest syndrome occurs in 15-43% of patients with sickle cell disease. Individuals
with sickle cell disease not only have problems with their complement system, but they also have functional
asplenia, which predisposes them to infection with encapsulated organisms such as S pneumoniae and H
influenzae type B.
emedicine.medscape.com/article/967822-overview
7/12
1/11/15
Pediatric Pneumonia
Mortality
The United Nations Children's Fund (UNICEF) estimates that 3 million children die worldwide from pneumonia each
year; these deaths almost exclusively occur in children with underlying conditions, such as chronic lung disease
of prematurity, congenital heart disease, and immunosuppression. Although most fatalities occur in developing
countries, pneumonia remains a significant cause of morbidity in industrialized nations.
According to the WHOs Global Burden of Disease 2000 Project, lower respiratory infections were the second
leading cause of death in children younger than 5 years (about 2.1 million [19.6%]).[24] Most children are treated
as outpatients and fully recover. However, in young infants and immunocompromised individuals, mortality is much
higher. In studies of adults with pneumonia, a higher mortality rate is associated with abnormal vital signs,
immunodeficiency, and certain pathogens.
Patient Education
Counsel parents regarding the need to prevent exposure of infants to tobacco smoke, and, as part of anticipatory
primary care, educate parents regarding later infectious exposures in daycare centers, schools, and similar
settings as well as the importance of hand washing. In addition, discuss the benefit infants may receive from
pneumococcal immunization and annual influenza immunization and the potential benefits and costs of RSV
immune globulin (see Prevention). Emphasize careful longitudinal surveillance for long-term problems with growth,
development, otitis, reactive airway disease, and other complications.
Most children treated with outpatient antibiotics are much improved within 48 hours after the initiation of treatment.
Educate parents about and caution them to look for the signs of increasing respiratory distress and to seek
medical attention immediately should any of these signs appear.
For excellent patient education resources, visit eMedicineHealth's Lung Disease and Respiratory Health Center.
Also, see eMedicineHealth's patient education articles Bronchoscopy, Viral Pneumonia, and Bacterial Pneumonia.
Contributor Information and Disclosures
Author
Nicholas John Bennett, MBBCh, PhD, MA(Cantab), FAAP Assistant Professor of Pediatrics, Co-Director of
Antimicrobial Stewardship, Medical Director, Division of Pediatric Infectious Diseases and Immunology,
Connecticut Children's Medical Center
Nicholas John Bennett, MBBCh, PhD, MA(Cantab), FAAP is a member of the following medical societies:
Alpha Omega Alpha and American Academy of Pediatrics
Disclosure: Nothing to disclose.
Coauthor(s)
Joseph Domachowske, MD Professor of Pediatrics, Microbiology and Immunology, Department of Pediatrics,
Division of Infectious Diseases, State University of New York Upstate Medical University
Joseph Domachowske, MD is a member of the following medical societies: Alpha Omega Alpha, American
Academy of Pediatrics, American Society for Microbiology, Infectious Diseases Society of America, Pediatric
Infectious Diseases Society, and Phi Beta Kappa
Disclosure: Nothing to disclose.
Chief Editor
Russell W Steele, MD Head, Division of Pediatric Infectious Diseases, Ochsner Children's Health Center;
Clinical Professor, Department of Pediatrics, Tulane University School of Medicine
Russell W Steele, MD is a member of the following medical societies: American Academy of Pediatrics,
American Association of Immunologists, American Pediatric Society, American Society for Microbiology,
Infectious Diseases Society of America, Louisiana State Medical Society, Pediatric Infectious Diseases
Society, Society for Pediatric Research, and Southern Medical Association
Disclosure: Nothing to disclose.
Additional Contributors
Leslie L Barton, MD Professor Emerita of Pediatrics, University of Arizona College of Medicine
Leslie L Barton, MD is a member of the following medical societies: American Academy of Pediatrics,
Association of Pediatric Program Directors, Infectious Diseases Society of America, and Pediatric Infectious
Diseases Society
Disclosure: Nothing to disclose.
Heidi Connolly, MD Associate Professor of Pediatrics and Psychiatry, University of Rochester School of
Medicine and Dentistry; Director, Pediatric Sleep Medicine Services, Strong Sleep Disorders Center
Disclosure: Nothing to disclose.
Brent R King , MD, MMM Clive Nancy and Pierce Runnells Distinguished Professor of Emergency Medicine;
Professor of Pediatrics, University of Texas Health Science Center at Houston; Chair, Department of
Emergency Medicine, Chief of Emergency Services, Memorial Hermann Hospital and LBJ Hospital
Disclosure: Nothing to disclose.
Jeff L Myers, MD, PhD Chief, Pediatric and Congenital Cardiac Surgery, Department of Surgery,
Massachusetts General Hospital; Associate Professor of Surgery, Harvard Medical School
emedicine.medscape.com/article/967822-overview
8/12
1/11/15
Pediatric Pneumonia
Disclosure: Nothing to disclose.
Mark I Neuman, MD, MPH Assistant Professor of Pediatrics, Harvard Medical School; Attending Physician,
Division of Emergency Medicine, Children's Hospital Boston
Mark I Neuman, MD, MPH is a member of the following medical societies: Society for Pediatric Research
Disclosure: Nothing to disclose.
Jos Rafael Romero, MD Director of Pediatric Infectious Diseases Fellowship Program, Associate Professor,
Department of Pediatrics, Combined Division of Pediatric Infectious Diseases, Creighton University/University of
Nebraska Medical Center
Jos Rafael Romero, MD is a member of the following medical societies: American Academy of Pediatrics,
American Society for Microbiology, Infectious Diseases Society of America, New York Academy of Sciences,
and Pediatric Infectious Diseases Society
Disclosure: Nothing to disclose.
Manika Suryadevara, MD Fellow in Pediatric Infectious Diseases, Department of Pediatrics, State University
of New York Upstate Medical University
Disclosure: Nothing to disclose.
Isabel Virella-Lowell, MD Department of Pediatrics, Division of Pulmonary Diseases, Pediatric Pulmonology,
Allergy and Immunology
Disclosure: Nothing to disclose.
Garry Wilkes, MBBS, FACEM Director of Emergency Medicine, Calvary Hospital, Canberra, ACT; Adjunct
Associate Professor, Edith Cowan University, Western Australia
Disclosure: Nothing to disclose.
Mary L Windle, PharmD Adjunct Associate Professor, University of Nebraska Medical Center College of
Pharmacy; Editor-in-Chief, Medscape Drug Reference
Disclosure: Nothing to disclose.
Grace M Young, MD Associate Professor, Department of Pediatrics, University of Maryland Medical Center
Disclosure: Nothing to disclose.
References
1. Douglas D. Twice-Daily Amoxicillin Effective in Children With Pneumonia. Medscape Medical News.
Available at http://www.medscape.com/viewarticle/823469. Accessed April 22, 2014.
2. Vilas-Boas AL, Fontoura MS, Xavier-Souza G, Arajo-Neto CA, Andrade SC, Brim RV, et al. Comparison
of oral amoxicillin given thrice or twice daily to children between 2 and 59 months old with non-severe
pneumonia: a randomized controlled trial. J Antimicrob Chemother. Mar 19 2014;[Medline].
3. Boggs W. Point-of-Care Ultrasound Diagnoses Pneumonia in Children. Medscape Medical News.
December 10, 2012. Available at http://www.medscape.com/viewarticle/775961. Accessed January 9,
2013.
4. Shah VP, Tunik MG, Tsung JW. Prospective Evaluation of Point-of-Care Ultrasonography for the
Diagnosis of Pneumonia in Children and Young Adults. Arch Pediatr Adolesc Med. Dec 10 2012;1-7.
[Medline].
5. Metinko AP. Neonatal pulmonary host defense mechanisms. In: Polin RA, Fox WW, eds. Fetal and
Neonatal Physiology. 3rd ed. Philadelphia, Pa: WB Saunders Co; 2004:1620-73.
6. Barnett ED, Klein JO. Bacterial infections of the respiratory tract. In: Remington JS, Klein JO, eds.
Infectious Diseases of the Fetus and Newborn Infant. 6th ed. Philadelphia, Pa: Elsevier Saunders Co;
2006:297-317.
7. Bone RC, Grodzin CJ, Balk RA. Sepsis: a new hypothesis for pathogenesis of the disease process.
Chest. Jul 1997;112(1):235-43. [Medline].
8. Michelow IC, Olsen K, Lozano J, Rollins NK, Duffy LB, Ziegler T, et al. Epidemiology and clinical
characteristics of community-acquired pneumonia in hospitalized children. Pediatrics. Apr
2004;113(4):701-7. [Medline].
9. Stoll BJ, Hansen NI, Higgins RD, Fanaroff AA, Duara S, Goldberg R, et al. Very low birth weight preterm
infants with early onset neonatal sepsis: the predominance of gram-negative infections continues in the
National Institute of Child Health and Human Development Neonatal Research Network, 2002-2003.
Pediatr Infect Dis J. Jul 2005;24(7):635-9. [Medline].
10. Mishaan AM, Mason EO Jr, Martinez-Aguilar G, Hammerman W, Propst JJ, Lupski JR, et al. Emergence
of a predominant clone of community-acquired Staphylococcus aureus among children in Houston,
Texas. Pediatr Infect Dis J. Mar 2005;24(3):201-6. [Medline].
11. Kotecha S, Hodge R, Schaber JA, Miralles R, Silverman M, Grant WD. Pulmonary Ureaplasma
urealyticum is associated with the development of acute lung inflammation and chronic lung disease in
preterm infants. Pediatr Res. Jan 2004;55(1):61-8. [Medline].
emedicine.medscape.com/article/967822-overview
9/12
1/11/15
Pediatric Pneumonia
12. Katz B, Patel P, Duffy L, Schelonka RL, Dimmitt RA, Waites KB. Characterization of ureaplasmas
isolated from preterm infants with and without bronchopulmonary dysplasia. J Clin Microbiol. Sep
2005;43(9):4852-4. [Medline]. [Full Text].
13. Heggie AD, Bar-Shain D, Boxerbaum B, Fanaroff AA, O'Riordan MA, Robertson JA. Identification and
quantification of ureaplasmas colonizing the respiratory tract and assessment of their role in the
development of chronic lung disease in preterm infants. Pediatr Infect Dis J. Sep 2001;20(9):854-9.
[Medline].
14. Ballard HO, Bernard P, Whitehead V, et al. Determining the incidence of Ureaplasma spp. and its role in
development of bronchopulmonary dysplasia. [Abstract 3858.111]. Pediatric Academic Societies Meeting
2009. Baltimore, MD. May 3, 2009. aps-spr.org. Available at
http://www.abstracts2view.com/pas/view.php?nu=PAS09L1_3037. Accessed November 5, 2010.
15. Tsolia MN, Psarras S, Bossios A, Audi H, Paldanius M, Gourgiotis D, et al. Etiology of communityacquired pneumonia in hospitalized school-age children: evidence for high prevalence of viral infections.
Clin Infect Dis. Sep 1 2004;39(5):681-6. [Medline].
16. Nascimento-Carvalho CM, Ribeiro CT, Cardoso MR, Barral A, Arajo-Neto CA, Oliveira JR, et al. The role
of respiratory viral infections among children hospitalized for community-acquired pneumonia in a
developing country. Pediatr Infect Dis J. Oct 2008;27(10):939-41. [Medline].
17. Juvn T, Mertsola J, Waris M, Leinonen M, Meurman O, Roivainen M, et al. Etiology of communityacquired pneumonia in 254 hospitalized children. Pediatr Infect Dis J. Apr 2000;19(4):293-8. [Medline].
18. [Guideline] American Academy of Pediatrics Committee on Infectious Diseases. Recommended
childhood and adolescent immunization schedules--United States, 2009. Pediatrics. Jan 2009;123(1):18990. [Medline].
19. Tajima T, Nakayama E, Kondo Y, Hirai F, Ito H, Iitsuka T, et al. Etiology and clinical study of communityacquired pneumonia in 157 hospitalized children. J Infect Chemother. Dec 2006;12(6):372-9. [Medline].
20. Denny FW, Clyde WA Jr. Acute lower respiratory tract infections in nonhospitalized children. J Pediatr.
May 1986;108(5 Pt 1):635-46. [Medline].
21. Thompson WW, Shay DK, Weintraub E, Brammer L, Bridges CB, Cox NJ, et al. Influenza-associated
hospitalizations in the United States. JAMA. Sep 15 2004;292(11):1333-40. [Medline].
22. Black SB, Shinefield HR, Ling S, Hansen J, Fireman B, Spring D, et al. Effectiveness of heptavalent
pneumococcal conjugate vaccine in children younger than five years of age for prevention of pneumonia.
Pediatr Infect Dis J. Sep 2002;21(9):810-5. [Medline].
23. Li ST, Tancredi DJ. Empyema hospitalizations increased in US children despite pneumococcal conjugate
vaccine. Pediatrics. Jan 2010;125(1):26-33. [Medline].
24. Rudan I, Tomaskovic L, Boschi-Pinto C, Campbell H. Global estimate of the incidence of clinical
pneumonia among children under five years of age. Bull World Health Organ. Dec 2004;82(12):895-903.
[Medline]. [Full Text].
25. Shah S, Bachur R, Kim D, Neuman MI. Lack of predictive value of tachypnea in the diagnosis of
pneumonia in children. Pediatr Infect Dis J. May 2010;29(5):406-9. [Medline].
26. Wingerter SL, Bachur RG, Monuteaux MC, Neuman MI. Application of the World Health Organization
Criteria to Predict Radiographic Pneumonia in a US-based Pediatric Emergency Department. Pediatr
Infect Dis J. Jun 2012;31(6):561-4. [Medline].
27. Lynch T, Platt R, Gouin S, Larson C, Patenaude Y. Can we predict which children with clinically
suspected pneumonia will have the presence of focal infiltrates on chest radiographs?. Pediatrics. Mar
2004;113(3 Pt 1):e186-9. [Medline].
28. Mahabee-Gittens EM, Grupp-Phelan J, Brody AS, Donnelly LF, Bracey SE, Duma EM, et al. Identifying
children with pneumonia in the emergency department. Clin Pediatr (Phila). Jun 2005;44(5):427-35.
[Medline].
29. Rothrock SG, Green SM, Fanelli JM, Cruzen E, Costanzo KA, Pagane J. Do published guidelines predict
pneumonia in children presenting to an urban ED?. Pediatr Emerg Care. Aug 2001;17(4):240-3. [Medline].
30. Bachur R, Perry H, Harper MB. Occult pneumonias: empiric chest radiographs in febrile children with
leukocytosis. Ann Emerg Med. Feb 1999;33(2):166-73. [Medline].
31. Murphy CG, van de Pol AC, Harper MB, Bachur RG. Clinical predictors of occult pneumonia in the febrile
child. Acad Emerg Med. Mar 2007;14(3):243-9. [Medline].
32. Rutman MS, Bachur R, Harper MB. Radiographic pneumonia in young, highly febrile children with
leukocytosis before and after universal conjugate pneumococcal vaccination. Pediatr Emerg Care. Jan
2009;25(1):1-7. [Medline].
33. Wubbel L, Muniz L, Ahmed A, Trujillo M, Carubelli C, McCoig C, et al. Etiology and treatment of
community-acquired pneumonia in ambulatory children. Pediatr Infect Dis J. Feb 1999;18(2):98-104.
[Medline].
34. Waris ME, Toikka P, Saarinen T, Nikkari S, Meurman O, Vainionp R, et al. Diagnosis of Mycoplasma
pneumoniae pneumonia in children. J Clin Microbiol. Nov 1998;36(11):3155-9. [Medline]. [Full Text].
35. Chaaban H, Singh K, Huang J, Siryaporn E, Lim YP, Padbury JF. The role of inter-alpha inhibitor proteins
in the diagnosis of neonatal sepsis. J Pediatr. Apr 2009;154(4):620-622.e1. [Medline].
emedicine.medscape.com/article/967822-overview
10/12
1/11/15
Pediatric Pneumonia
36. Blaschke AJ, Heyrend C, Byington CL, Obando I, Vazquez-Barba I, Doby EH, et al. Molecular analysis
improves pathogen identification and epidemiologic study of pediatric parapneumonic empyema. Pediatr
Infect Dis J. Apr 2011;30(4):289-94. [Medline]. [Full Text].
37. Neuman MI, Harper MB. Evaluation of a rapid urine antigen assay for the detection of invasive
pneumococcal disease in children. Pediatrics. Dec 2003;112(6 Pt 1):1279-82. [Medline].
38. Sherman MP, Goetzman BW, Ahlfors CE, Wennberg RP. Tracheal asiration and its clinical correlates in
the diagnosis of congenital pneumonia. Pediatrics. Feb 1980;65(2):258-63. [Medline].
39. Gauvin F, Dassa C, Chabou M, Proulx F, Farrell CA, Lacroix J. Ventilator-associated pneumonia in
intubated children: comparison of different diagnostic methods. Pediatr Crit Care Med. Oct 2003;4(4):43743. [Medline].
40. Gauvin F, Lacroix J, Guertin MC, Proulx F, Farrell CA, Moghrabi A, et al. Reproducibility of blind
protected bronchoalveolar lavage in mechanically ventilated children. Am J Respir Crit Care Med. Jun 15
2002;165(12):1618-23. [Medline].
41. Labenne M, Poyart C, Rambaud C, Goldfarb B, Pron B, Jouvet P, et al. Blind protected specimen brush
and bronchoalveolar lavage in ventilated children. Crit Care Med. Nov 1999;27(11):2537-43. [Medline].
42. Falade AG, Mulholland EK, Adegbola RA, Greenwood BM. Bacterial isolates from blood and lung aspirate
cultures in Gambian children with lobar pneumonia. Ann Trop Paediatr. Dec 1997;17(4):315-9. [Medline].
43. Klein JO. Diagnostic lung puncture in the pneumonias of infants and children. Pediatrics. Oct
1969;44(4):486-92. [Medline].
44. Wigglesworth JS. Perinatal Pathology. 2nd ed. Philadelphia, Pa: WB Saunders Co; 1996:131-57, 184-7.
45. Bradley JS, Byington CL, Shah SS, et al. The management of community-acquired pneumonia in infants
and children older than 3 months of age: clinical practice guidelines by the pediatric infectious diseases
society and the infectious diseases society of america. Clin Infect Dis. Oct 2011;53(7):e25-76. [Medline].
46. Willwerth BM, Harper MB, Greenes DS. Identifying hospitalized infants who have bronchiolitis and are at
high risk for apnea. Ann Emerg Med. Oct 2006;48(4):441-7. [Medline].
47. Muszynski JA, Knatz NL, Sargel CL, Fernandez SA, Marquardt DJ, Hall MW. Timing of correct parenteral
antibiotic initiation and outcomes from severe bacterial community-acquired pneumonia in children.
Pediatr Infect Dis J. Apr 2011;30(4):295-301. [Medline].
48. Cincinnati Children's Hospital Medical Center. Evidence based care guideline for community acquired
pneumonia in children 60 days through 17 years of age. Cincinnati (OH): Cincinnati Children's Hospital
Medical Center. Jul. 2006. Available at http://guideline.gov/index.aspx. Accessed September 22, 2010.
49. Neuman MI, Kelley M, Harper MB, File TM Jr, Camargo CA Jr. Factors associated with antimicrobial
resistance and mortality in pneumococcal bacteremia. J Emerg Med. May 2007;32(4):349-57. [Medline].
[Full Text].
50. Barber J Jr. Narrow-Spectrum Antibiotics Effective for Pediatric Pneumonia. Medscape Medical News
[serial online]. Oct 29 2013;Accessed Nov 6 2013. Available at
http://www.medscape.com/viewarticle/813449.
51. Williams DJ, Hall M, Shah SS, et al. Narrow Vs broad-spectrum antimicrobial therapy for children
hospitalized with pneumonia. Pediatrics. Nov 2013;132(5):e1141-8. [Medline].
52. Braude AC, Hornstein A, Klein M, Vas S, Rebuck AS. Pulmonary disposition of tobramycin. Am Rev
Respir Dis. May 1983;127(5):563-5. [Medline].
53. Pennington JE. Penetration of antibiotics into respiratory secretions. Rev Infect Dis. Jan-Feb
1981;3(1):67-73. [Medline].
54. Clark RH, Bloom BT, Spitzer AR, Gerstmann DR. Empiric use of ampicillin and cefotaxime, compared
with ampicillin and gentamicin, for neonates at risk for sepsis is associated with an increased risk of
neonatal death. Pediatrics. Jan 2006;117(1):67-74. [Medline].
55. Siempos II, Vardakas KZ, Kopterides P, Falagas ME. Adjunctive therapies for community-acquired
pneumonia: a systematic review. J Antimicrob Chemother. Oct 2008;62(4):661-8. [Medline].
56. Black S, Shinefield H, Fireman B, Lewis E, Ray P, Hansen JR, et al. Efficacy, safety and immunogenicity
of heptavalent pneumococcal conjugate vaccine in children. Northern California Kaiser Permanente
Vaccine Study Center Group. Pediatr Infect Dis J. Mar 2000;19(3):187-95. [Medline].
57. FDA. FDA Approves Pneumococcal Disease Vaccine with Broader Protection. February 24, 2010.
Available at http://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm201758.htm. Accessed
September 22, 2010.
58. Lassi ZS, Haider BA, Bhutta ZA. Zinc supplementation for the prevention of pneumonia in children aged 2
months to 59 months. Cochrane Database Syst Rev. Dec 8 2010;CD005978. [Medline].
59. Addo-Yobo E, Chisaka N, Hassan M, Hibberd P, Lozano JM, Jeena P, et al. Oral amoxicillin versus
injectable penicillin for severe pneumonia in children aged 3 to 59 months: a randomised multicentre
equivalency study. Lancet. Sep 25-Oct 1 2004;364(9440):1141-8. [Medline].
60. Brasfield DM, Stagno S, Whitley RJ, Cloud G, Cassell G, Tiller RE. Infant pneumonitis associated with
cytomegalovirus, Chlamydia, Pneumocystis, and Ureaplasma: follow-up. Pediatrics. Jan 1987;79(1):7683. [Medline].
emedicine.medscape.com/article/967822-overview
11/12
1/11/15
Pediatric Pneumonia
61. Brewster DR, De Silva LM, Henry RL. Chlamydia trachomatis and respiratory disease in infants. Med J
Aust. Oct 3 1981;2(7):328-30. [Medline].
62. Cevey-Macherel M, Galetto-Lacour A, Gervaix A, Siegrist CA, Bille J, Bescher-Ninet B, et al. Etiology of
community-acquired pneumonia in hospitalized children based on WHO clinical guidelines. Eur J Pediatr.
Dec 2009;168(12):1429-36. [Medline].
63. Courtoy I, Lande AE, Turner RB. Accuracy of radiographic differentiation of bacterial from nonbacterial
pneumonia. Clin Pediatr (Phila). Jun 1989;28(6):261-4. [Medline].
64. de Man P, Verhoeven BA, Verbrugh HA, Vos MC, van den Anker JN. An antibiotic policy to prevent
emergence of resistant bacilli. Lancet. Mar 18 2000;355(9208):973-8. [Medline].
65. Fasoli L, Paldanius M, Don M, Valent F, Vetrugno L, Korppi M, et al. Simkania negevensis in communityacquired pneumonia in Italian children. Scand J Infect Dis. 2008;40(3):269-72. [Medline].
66. Gckel C, Benz-Bohm G, Widemann B. Mycoplasmal pneumonias in childhood. Roentgen features,
differential diagnosis and review of literature. Pediatr Radiol. 1989;19(8):499-503. [Medline].
67. Haney PJ, Bohlman M, Sun CC. Radiographic findings in neonatal pneumonia. AJR Am J Roentgenol. Jul
1984;143(1):23-6. [Medline].
68. Hansen J, Black S, Shinefield H, Cherian T, Benson J, Fireman B, et al. Effectiveness of heptavalent
pneumococcal conjugate vaccine in children younger than 5 years of age for prevention of pneumonia:
updated analysis using World Health Organization standardized interpretation of chest radiographs.
Pediatr Infect Dis J. Sep 2006;25(9):779-81. [Medline].
69. Korppi M, Kiekara O, Heiskanen-Kosma T, Soimakallio S. Comparison of radiological findings and
microbial aetiology of childhood pneumonia. Acta Paediatr. Apr 1993;82(4):360-3. [Medline].
70. Mathews B, Shah S, Cleveland RH, Lee EY, Bachur RG, Neuman MI. Clinical predictors of pneumonia
among children with wheezing. Pediatrics. Jul 2009;124(1):e29-36. [Medline].
71. Puumalainen T, Quiambao B, Abucejo-Ladesma E, Lupisan S, Heiskanen-Kosma T, Ruutu P, et al.
Clinical case review: a method to improve identification of true clinical and radiographic pneumonia in
children meeting the World Health Organization definition for pneumonia. BMC Infect Dis. Jul 21
2008;8:95. [Medline]. [Full Text].
72. Radkowski MA, Kranzler JK, Beem MO, Tipple MA. Chlamydia pneumonia in infants: radiography in 125
cases. AJR Am J Roentgenol. Oct 1981;137(4):703-6. [Medline].
73. Wahlgren H, Mortensson W, Eriksson M, Finkel Y, Forsgren M, Leinonen M. Radiological findings in
children with acute pneumonia: age more important than infectious agent. Acta Radiol. Jul
2005;46(4):431-6. [Medline].
74. Wildin SR, Chonmaitree T, Swischuk LE. Roentgenographic features of common pediatric viral respiratory
tract infections. Am J Dis Child. Jan 1988;142(1):43-6. [Medline].
75. Wolf DG, Greenberg D, Shemer-Avni Y, Givon-Lavi N, Bar-Ziv J, Dagan R. Association of human
metapneumovirus with radiologically diagnosed community-acquired alveolar pneumonia in young
children. J Pediatr. Jan 2010;156(1):115-20. [Medline].
76. World Health Organization. Handbook. IMCI integrated management of childhood illness. Available at
http://whqlibdoc.who.int/publications/2005/9241546441.pdf. Accessed November 5,2010.
Medscape Reference 2011 WebMD, LLC
emedicine.medscape.com/article/967822-overview
12/12
You might also like
- Case Study PneumoniaDocument53 pagesCase Study PneumoniaWilliam Agoncillo100% (1)
- Essential Update: Pediatric Pneumonia May Be Effectively Treated With Twice-Daily AmoxicillinDocument54 pagesEssential Update: Pediatric Pneumonia May Be Effectively Treated With Twice-Daily AmoxicillinYostesara Maurena SantosaNo ratings yet
- Pneumonia: Key FactsDocument28 pagesPneumonia: Key FactsAri Widiastuti NiPutuNo ratings yet
- Management of Tuberculosis: A guide for clinicians (eBook edition)From EverandManagement of Tuberculosis: A guide for clinicians (eBook edition)No ratings yet
- Case Study PcapDocument3 pagesCase Study PcapClaire PalaciosNo ratings yet
- Practice Essentials: Pediatric Pneumonia MedicationDocument56 pagesPractice Essentials: Pediatric Pneumonia MedicationAnonymous HgX3mN1oNo ratings yet
- Tuberculous MeningitisDocument11 pagesTuberculous MeningitiszuhriNo ratings yet
- Case Studies - Tetralogy of FallotDocument16 pagesCase Studies - Tetralogy of FallotKunwar Sidharth SaurabhNo ratings yet
- PGI MANIMTIM - COVID-19 in PregnancyDocument1 pagePGI MANIMTIM - COVID-19 in PregnancyKim Adarem Joy ManimtimNo ratings yet
- Ward Case PresentationDocument92 pagesWard Case PresentationSuzette Rae TateNo ratings yet
- GlomerulonephritisDocument35 pagesGlomerulonephritisapi-19916399No ratings yet
- TB Case StudyDocument2 pagesTB Case StudyReisabelle LabianoNo ratings yet
- Pulmonary TuberculosisDocument46 pagesPulmonary Tuberculosisroseann_808100% (1)
- Pneumonia - Case Pres.Document35 pagesPneumonia - Case Pres.wew33380% (5)
- PneumoniaDocument26 pagesPneumonialovelots1234No ratings yet
- A Case Study On Graves DiseaseDocument46 pagesA Case Study On Graves DiseaseRenie SerranoNo ratings yet
- Communicable DiseaseDocument3 pagesCommunicable Diseasemiss RNNo ratings yet
- Pneumonia: Neonates To AdolescentsDocument32 pagesPneumonia: Neonates To AdolescentsAthenaTudino100% (2)
- Pathophysiology of Covid-19 Infection: What Is The Novel Coronavirus (Sars-Cov-2) Doing To Body? A Comprehensive Systematic ReviewDocument15 pagesPathophysiology of Covid-19 Infection: What Is The Novel Coronavirus (Sars-Cov-2) Doing To Body? A Comprehensive Systematic ReviewMade DeanaNo ratings yet
- BRONCHITIS Case PresentationDocument28 pagesBRONCHITIS Case PresentationJoshua DulayNo ratings yet
- MDRTB Case StudyDocument35 pagesMDRTB Case StudyFejlean Angelica AntineoNo ratings yet
- ENCEPHALITISDocument104 pagesENCEPHALITISAsogaa MeteranNo ratings yet
- Pathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionDocument2 pagesPathognomonic Signs of Communicable Diseases: JJ8009 Health & NutritionMauliza Resky NisaNo ratings yet
- Febrile SeizureDocument6 pagesFebrile SeizurepipimseptianaNo ratings yet
- Erythroblastosis Case StudyDocument19 pagesErythroblastosis Case StudyMaricel Agcaoili GallatoNo ratings yet
- Pyloric StenosisDocument5 pagesPyloric Stenosisensoooooooooo100% (1)
- Knowledge, Attitude and Practices On Vaccination During Time of Pandemic Among Pediatrician of Olongapo City, Zambales, PhilippinesDocument15 pagesKnowledge, Attitude and Practices On Vaccination During Time of Pandemic Among Pediatrician of Olongapo City, Zambales, PhilippinesNiran ThapaNo ratings yet
- Final Case Study Subgroup 1 PneumoniaDocument80 pagesFinal Case Study Subgroup 1 PneumoniaCyril SolimanNo ratings yet
- Lack of Insulin Decreases Available Glucose For CellDocument1 pageLack of Insulin Decreases Available Glucose For CellvicenteturasNo ratings yet
- Malaria PreventionDocument3 pagesMalaria PreventionRohit_Patkar_2942No ratings yet
- Stevens Johnson SyndromeDocument6 pagesStevens Johnson SyndromeAudrey LeonarNo ratings yet
- TB MeningitisDocument46 pagesTB MeningitishenniwtNo ratings yet
- Thyroid Papillary Carcinoma CaseDocument6 pagesThyroid Papillary Carcinoma CaseRandy F BabaoNo ratings yet
- Pneumonia CaseDocument11 pagesPneumonia CaseBrigette Molly LopezNo ratings yet
- Pediatric PneumoniaDocument3 pagesPediatric PneumoniaErika GardeNo ratings yet
- Broncho PneumoniaDocument46 pagesBroncho PneumoniaAfrianzah Sevenfoldism100% (1)
- Exudative Pleural Effusions - UpToDateDocument2 pagesExudative Pleural Effusions - UpToDateAsif IqbalNo ratings yet
- Lung AbscessDocument27 pagesLung AbscessMalueth Angui100% (1)
- Health Info Health Info Medicines Advanced Search Register Login Top of Form User NameDocument24 pagesHealth Info Health Info Medicines Advanced Search Register Login Top of Form User NameAnusha PradhanNo ratings yet
- Case 1 (Pneumonia) ArioDocument26 pagesCase 1 (Pneumonia) ArioJoegie ArioNo ratings yet
- Poststreptococcal Glomerulonephritis - UpToDateDocument21 pagesPoststreptococcal Glomerulonephritis - UpToDateHandre Putra100% (1)
- Teddy Essel Thesis Final PDFDocument59 pagesTeddy Essel Thesis Final PDFAltaf KhaanNo ratings yet
- Pathology Polycystic Kidney DiseaseDocument4 pagesPathology Polycystic Kidney DiseaseOnyedika EgbujoNo ratings yet
- Acute Bronchiolitis: Zakaria Omar Elzwie Najwa Abdulallah Alfergany (Mub) NovemberDocument28 pagesAcute Bronchiolitis: Zakaria Omar Elzwie Najwa Abdulallah Alfergany (Mub) Novemberزكريا عمرNo ratings yet
- PTB Case StudyDocument6 pagesPTB Case StudyTrisha Carolina SottoNo ratings yet
- Hand Foot & Mouth DiseaseDocument23 pagesHand Foot & Mouth DiseaseKabang Moa100% (1)
- Biliary AtresiaDocument25 pagesBiliary Atresiajulius billiNo ratings yet
- FBCDocument14 pagesFBCJane GarciaNo ratings yet
- Bronchiolitis Clinical Practice GuidelineDocument21 pagesBronchiolitis Clinical Practice GuidelineJuwita PratiwiNo ratings yet
- Pa Tho Physiology Chicken PoxDocument4 pagesPa Tho Physiology Chicken PoxPao RamirezNo ratings yet
- Case StudyDocument84 pagesCase Studyalcojonic0% (1)
- Case Presentation Hepatitis A LuluDocument28 pagesCase Presentation Hepatitis A LuluBrenda KarinaNo ratings yet
- Case Study Burn Injury - 11Document15 pagesCase Study Burn Injury - 11Evelyn MedinaNo ratings yet
- The Effectiveness of Educational Program On Nurses' Competencies Regarding Pre-Eclampsia Care in Three Hospitals in Sudan2021Document6 pagesThe Effectiveness of Educational Program On Nurses' Competencies Regarding Pre-Eclampsia Care in Three Hospitals in Sudan2021International Journal of Innovative Science and Research Technology100% (1)
- Pneumonia Case StudyDocument8 pagesPneumonia Case StudyChristopher John AgueloNo ratings yet
- Listeria Monocytogenes Escherichia Coli: Signs and SymptomsDocument15 pagesListeria Monocytogenes Escherichia Coli: Signs and SymptomsPuput's BourboneNo ratings yet
- 2002 23 132 Benjamin Gaston: Pediatr. RevDocument11 pages2002 23 132 Benjamin Gaston: Pediatr. RevDiego DíazNo ratings yet
- Proposal To Include Antibacterial Drugs For Treating Upper and Lower Respiratory Infections in ChildrenDocument52 pagesProposal To Include Antibacterial Drugs For Treating Upper and Lower Respiratory Infections in ChildrenAznil FajriNo ratings yet
- Updated September 2016: PneumoniaDocument5 pagesUpdated September 2016: PneumoniaYidnekachew Girma Assefa100% (1)
- Necrotizing FasciitisDocument5 pagesNecrotizing Fasciitisnsl1225No ratings yet
- Swine DiseaseDocument38 pagesSwine DiseasehapipillyelloNo ratings yet
- Flu Guide For Parents 2021Document2 pagesFlu Guide For Parents 2021api-256233875No ratings yet
- Plasmodium: 25/02/2019 Ss NghoshiDocument31 pagesPlasmodium: 25/02/2019 Ss NghoshiJohanna HaludiluNo ratings yet
- Pathogenesis Typhoid Fever PDFDocument7 pagesPathogenesis Typhoid Fever PDFAry Nahdiyani Amalia100% (1)
- Test Bank For Pathophysiology 6th Edition by BanasikDocument5 pagesTest Bank For Pathophysiology 6th Edition by BanasikRobert Booth100% (35)
- Lab Report 2157646 20210113110650Document3 pagesLab Report 2157646 20210113110650marlon molinaNo ratings yet
- Sample: Georgia Department of Public HealthDocument1 pageSample: Georgia Department of Public HealthWSB-TV Assignment DeskNo ratings yet
- MyChart - Test Details PDFDocument3 pagesMyChart - Test Details PDFAnonymous iy0yzUJOOrNo ratings yet
- Outbreak Student Worksheet AnswersDocument9 pagesOutbreak Student Worksheet AnswersArlie Espeña DucducanNo ratings yet
- Luliconazole, A New Antifungal Against Candida Species Isolated From Different SourcesDocument5 pagesLuliconazole, A New Antifungal Against Candida Species Isolated From Different SourcesLina LimNo ratings yet
- Biohackers Handbook ImmunityDocument37 pagesBiohackers Handbook ImmunityDaniel PopNo ratings yet
- Blood Cells LabDocument7 pagesBlood Cells LabKameron WardNo ratings yet
- CELYN H. NATURAL MAPEH LESSON PLAN (MR - Gepitulan)Document6 pagesCELYN H. NATURAL MAPEH LESSON PLAN (MR - Gepitulan)Celyn NaturalNo ratings yet
- S81 - Ram Ratan Lab-Cc: DR Sushrita Mukherjee DCP, Pathology Chief of Laboratory DR Lal Pathlabs LTDDocument2 pagesS81 - Ram Ratan Lab-Cc: DR Sushrita Mukherjee DCP, Pathology Chief of Laboratory DR Lal Pathlabs LTDCHANDAN KUMARNo ratings yet
- Lecture 27-Epizoonosis-Dr. Agnes Sri Siswati, SP - KK (K) (2020)Document45 pagesLecture 27-Epizoonosis-Dr. Agnes Sri Siswati, SP - KK (K) (2020)jasmine amaliaNo ratings yet
- Toxoplasmosis During PregnancyDocument4 pagesToxoplasmosis During PregnancyabhagaurNo ratings yet
- Historical Aspects of ImmunologyDocument14 pagesHistorical Aspects of ImmunologyKashishNo ratings yet
- WBC DisordersDocument45 pagesWBC DisordersyalahopaNo ratings yet
- Reading Comprehension Blood PC3Document4 pagesReading Comprehension Blood PC3Erik J. Roshan FloresNo ratings yet
- Agreement of Body Donation and Consent FormDocument8 pagesAgreement of Body Donation and Consent FormYp 培培No ratings yet
- Vol20no11 PDF VersionDocument187 pagesVol20no11 PDF VersionjaquiapestaNo ratings yet
- 先天免疫学糖生物学Document673 pages先天免疫学糖生物学Wenbo Yan100% (1)
- Procalcitonin Guided Antibiotic TherapyDocument20 pagesProcalcitonin Guided Antibiotic TherapyhziglamNo ratings yet
- Curs5 Hematologie AnvDocument59 pagesCurs5 Hematologie AnvRaluca PăunaNo ratings yet
- History of 1918 Flu Pandemic: The 1918 H1N1 Virus Has Been Synthesized and EvaluatedDocument3 pagesHistory of 1918 Flu Pandemic: The 1918 H1N1 Virus Has Been Synthesized and EvaluatedVicente BaltazarNo ratings yet
- Diagram I Pathogenesis of Insulin Dependent DM (Type 1) : DiagramsDocument2 pagesDiagram I Pathogenesis of Insulin Dependent DM (Type 1) : Diagramskristel_nicole18yahoNo ratings yet
- 1991 - de Groot Et Al. - Affinity Purification of A Major and A Minor Allergen From Dog Extract Serologic Activity of Affinity-Purified CanDocument10 pages1991 - de Groot Et Al. - Affinity Purification of A Major and A Minor Allergen From Dog Extract Serologic Activity of Affinity-Purified Canpond_1993No ratings yet
- Chapter 48 - Viruses Causing HepatitisDocument164 pagesChapter 48 - Viruses Causing HepatitisKevil LoriyaNo ratings yet
- OsteomyelitisDocument35 pagesOsteomyelitischinnnababu100% (1)