You might also like
- Completely Reverse Heart Disease With This Revolutionary TreatmentDocument8 pagesCompletely Reverse Heart Disease With This Revolutionary TreatmentSamee's Music100% (3)
- Obesity in Pregnancy - UPTO DATEComplications and Maternal Management - UpToDateDocument43 pagesObesity in Pregnancy - UPTO DATEComplications and Maternal Management - UpToDateCristinaCaprosNo ratings yet
- JanubDocument65 pagesJanubRoel PalmairaNo ratings yet
- Byol Meridian NewDocument2 pagesByol Meridian NewRahulKumar0% (1)
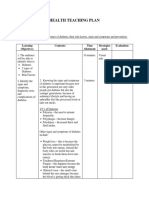
- Health Teaching Plan (Diabetes)Document6 pagesHealth Teaching Plan (Diabetes)Zam Pamate100% (1)
- Annotated Bibliography AssignmentDocument5 pagesAnnotated Bibliography Assignmentapi-242256465100% (2)
- Weaknes S/ Fatigue Polyphag IaDocument5 pagesWeaknes S/ Fatigue Polyphag IaEwert Hesketh Nillama PaquinganNo ratings yet
- OBESITY AND PREGNANCY OUTCOMESDocument5 pagesOBESITY AND PREGNANCY OUTCOMESAchmad Deza FaristaNo ratings yet
- Maternal Obesity, Gestational Hypertension, and Preterm DeliveryDocument8 pagesMaternal Obesity, Gestational Hypertension, and Preterm DeliveryGheavita Chandra DewiNo ratings yet
- Safety and Efficacy ofDocument11 pagesSafety and Efficacy ofJEFFERSON MUÑOZNo ratings yet
- Maternal Pregnancy Weight Gain and The Risk of Placental AbruptionDocument9 pagesMaternal Pregnancy Weight Gain and The Risk of Placental AbruptionMuhammad Aulia KurniawanNo ratings yet
- Informe 10Document8 pagesInforme 10karen paredes rojasNo ratings yet
- Jurnal ViolenceDocument6 pagesJurnal ViolenceIris BerlianNo ratings yet
- Percentage of Gestational Diabetes Mellitus Attributable To Overweight and ObesityDocument7 pagesPercentage of Gestational Diabetes Mellitus Attributable To Overweight and Obesitynunki aprillitaNo ratings yet
- Síndrome Metabólico (SM) en Niños y Adolescentes: Asociación Con Sensibilidad Insulínica (SI) y Con Magnitud y Distribución de La ObesidadDocument8 pagesSíndrome Metabólico (SM) en Niños y Adolescentes: Asociación Con Sensibilidad Insulínica (SI) y Con Magnitud y Distribución de La Obesidadgráficos furiososNo ratings yet
- Abed,+1114 Impacts+of+Dietary+Supplements+and+Nutrient Rich+Food+for+Pregnant+Women+on+Birth+Weight+in+Sugh+El Chmis Alkhoms+–+LiDocument8 pagesAbed,+1114 Impacts+of+Dietary+Supplements+and+Nutrient Rich+Food+for+Pregnant+Women+on+Birth+Weight+in+Sugh+El Chmis Alkhoms+–+LiLydia LuciusNo ratings yet
- Macrosmia and DMDocument4 pagesMacrosmia and DMAde Gustina SiahaanNo ratings yet
- Breast-Feeding and Risk For Childhood Obesity: Does Maternal Diabetes or Obesity Status Matter?Document7 pagesBreast-Feeding and Risk For Childhood Obesity: Does Maternal Diabetes or Obesity Status Matter?Dea Mustika HapsariNo ratings yet
- The Implications of Obesity On Pregnancy Outcome 2015 Obstetrics Gynaecology Reproductive MedicineDocument4 pagesThe Implications of Obesity On Pregnancy Outcome 2015 Obstetrics Gynaecology Reproductive MedicineNora100% (1)
- Risk factors for macrosomia in Latina womenDocument7 pagesRisk factors for macrosomia in Latina womenKhuriyatun NadhifahNo ratings yet
- Tugas Ebm Anisa Fitri HandaniDocument23 pagesTugas Ebm Anisa Fitri HandanianisFitrihandani anisaNo ratings yet
- Influence of Body Mass Index On The Incidence of Preterm LabourDocument6 pagesInfluence of Body Mass Index On The Incidence of Preterm LabourRizky MuharramNo ratings yet
- Diabetic MaternlaDocument4 pagesDiabetic MaternlaAde Gustina SiahaanNo ratings yet
- Its A Must To ReadDocument10 pagesIts A Must To ReadBNo ratings yet
- Bmi PregnancyDocument11 pagesBmi PregnancyLilik AnggrainiNo ratings yet
- Effect of inadequate weight gain in overweight and obese pregnant womenDocument3 pagesEffect of inadequate weight gain in overweight and obese pregnant womenainindyaNo ratings yet
- Jurnal PDFDocument5 pagesJurnal PDFWaica PratiwiNo ratings yet
- Obesidad en El EmbarazoDocument17 pagesObesidad en El Embarazodianaarias1703No ratings yet
- 08 AimukhametovaDocument10 pages08 AimukhametovahendraNo ratings yet
- Pre-Existing Diabetes Mellitus and Adverse PDFDocument5 pagesPre-Existing Diabetes Mellitus and Adverse PDFMetebNo ratings yet
- Maternal Factors For Low Birth Weight BabiesDocument3 pagesMaternal Factors For Low Birth Weight BabiesjanetNo ratings yet
- The Role of Parity in The Mode of DeliveryDocument11 pagesThe Role of Parity in The Mode of DeliveryKanuyasa GekzNo ratings yet
- Recém Ingressos Na UniversidadeDocument10 pagesRecém Ingressos Na UniversidadeanaflaviapfNo ratings yet
- Pattern of Glucose Intolerance Among Pregnant Women With Unexplained IUFDDocument5 pagesPattern of Glucose Intolerance Among Pregnant Women With Unexplained IUFDTri UtomoNo ratings yet
- Ni Hms 713785Document16 pagesNi Hms 713785mnn164No ratings yet
- Ansiedade, Qualidade Do Sono e Compulsão Alimentar em Adultos Com Sobrepeso Ou Obesidade PortuguesDocument8 pagesAnsiedade, Qualidade Do Sono e Compulsão Alimentar em Adultos Com Sobrepeso Ou Obesidade Portuguesviviane coelhoNo ratings yet
- Homa TannerDocument10 pagesHoma TannerClaudia VillablancaNo ratings yet
- Obesity in Children & Adolescents: Review ArticleDocument11 pagesObesity in Children & Adolescents: Review ArticleMatt QNo ratings yet
- Preconception Care ofDocument11 pagesPreconception Care ofsipen poltekkesbdgNo ratings yet
- Nutritional Status of Pre-School Children From Low Income FamiliesDocument11 pagesNutritional Status of Pre-School Children From Low Income FamiliesFiraz R AkbarNo ratings yet
- Managing Obesity in Malaysian Schools Are We Doing The Right StrategiesDocument9 pagesManaging Obesity in Malaysian Schools Are We Doing The Right StrategiesArushi GuptaNo ratings yet
- SX Metabólico en NiñosDocument8 pagesSX Metabólico en NiñosCésar Ayala GuzmánNo ratings yet
- Pregnancy nutrition guidelines for preconception through postpartumDocument16 pagesPregnancy nutrition guidelines for preconception through postpartumnanik setyawatiNo ratings yet
- Maternal Nutritional AssessmentDocument7 pagesMaternal Nutritional AssessmentchinchuNo ratings yet
- Literature Review Obesity in PregnancyDocument6 pagesLiterature Review Obesity in Pregnancyafmzbdjmjocdtm100% (1)
- Lactation and Maternal Risk of Type 2 Diabetes: A Population-Based StudyDocument6 pagesLactation and Maternal Risk of Type 2 Diabetes: A Population-Based StudyMoni SantamariaNo ratings yet
- Factors Associated With Fetal Macrosomia: ObjectiveDocument10 pagesFactors Associated With Fetal Macrosomia: ObjectiveAdib FraNo ratings yet
- Gestational Diabetes Mellitus: Science in MedicineDocument7 pagesGestational Diabetes Mellitus: Science in MedicineNatalia_p_mNo ratings yet
- A Word of Caution Against Excessive Protein IntakeDocument8 pagesA Word of Caution Against Excessive Protein IntakeBianca MickaelaNo ratings yet
- Abstract (Summary) : The Association Between Maternal Glucose Concentration and Child BMI at Age 3 YearsDocument7 pagesAbstract (Summary) : The Association Between Maternal Glucose Concentration and Child BMI at Age 3 YearsCedric Joshua BautistaNo ratings yet
- GDM Case StudyDocument5 pagesGDM Case Studydheeptha sundarNo ratings yet
- Malnutrition Among Pregnant Women Iran StudyDocument8 pagesMalnutrition Among Pregnant Women Iran StudyKimberlyjoycsolomonNo ratings yet
- 发表 修正Document2 pages发表 修正郑心洁No ratings yet
- Nutrition in The First 1000 Days: The Origin of Childhood ObesityDocument9 pagesNutrition in The First 1000 Days: The Origin of Childhood ObesityYoki VirgoNo ratings yet
- Muest RaDocument13 pagesMuest RaBruno LinoNo ratings yet
- Cardiovascular Disease Risk Factor (CVDRF) Associated Waist Circumference Patterns in Obese-Prone ChildrenDocument10 pagesCardiovascular Disease Risk Factor (CVDRF) Associated Waist Circumference Patterns in Obese-Prone ChildrenArmin Arceo DuranNo ratings yet
- Stir Rat 2014Document1 pageStir Rat 2014Dayana Cuyuche JuarezNo ratings yet
- Pengaruh Kenaikan Berat Badan Rata - Rata Per Minggu Pada Kehamilan Trimester Ii Dan Iii Terhadap Risiko Berat Bayi Lahir RendahDocument7 pagesPengaruh Kenaikan Berat Badan Rata - Rata Per Minggu Pada Kehamilan Trimester Ii Dan Iii Terhadap Risiko Berat Bayi Lahir Rendahmulia rahmaNo ratings yet
- Resumo: Artigos Originais / Original ArticlesDocument7 pagesResumo: Artigos Originais / Original ArticlesRafael SedlmaierNo ratings yet
- Pengaruh Kenaikan Berat Badan Rata - Rata Per Minggu Pada Kehamilan Trimester Ii Dan Iii Terhadap Risiko Berat Bayi Lahir RendahDocument7 pagesPengaruh Kenaikan Berat Badan Rata - Rata Per Minggu Pada Kehamilan Trimester Ii Dan Iii Terhadap Risiko Berat Bayi Lahir RendahmanalNo ratings yet
- Pregnancy Weight GainDocument9 pagesPregnancy Weight GainKevin MulyaNo ratings yet
- JAPI Body FatDocument6 pagesJAPI Body FatBhupendra MahantaNo ratings yet
- Metabolic Syndrome in Childhood: Association With Birth Weight, Maternal Obesity, and Gestational Diabetes MellitusDocument9 pagesMetabolic Syndrome in Childhood: Association With Birth Weight, Maternal Obesity, and Gestational Diabetes MellitusAnnisa FujiantiNo ratings yet
- Neck Circumference JOILANE 2020Document20 pagesNeck Circumference JOILANE 2020Joilane Alves Pereira FreireNo ratings yet
- Complementary and Alternative Medical Lab Testing Part 10: ObstetricsFrom EverandComplementary and Alternative Medical Lab Testing Part 10: ObstetricsNo ratings yet
- Medical Form Vehicle Licensing CharnwoodDocument12 pagesMedical Form Vehicle Licensing CharnwoodKalkin43No ratings yet
- Emailing Diabetic Wound Care White PaperDocument20 pagesEmailing Diabetic Wound Care White PaperGreatAkbar1No ratings yet
- Idf GDM Model of Care Implementation Protocol Guidelines For Healthcare ProfessionalsDocument20 pagesIdf GDM Model of Care Implementation Protocol Guidelines For Healthcare Professionalsdiabetes asiaNo ratings yet
- Himawan - BPJSDocument26 pagesHimawan - BPJSAndi Upik FathurNo ratings yet
- MCI Screening Test (FMGE) Question Paper - 2002Document678 pagesMCI Screening Test (FMGE) Question Paper - 2002Anbu Anbazhagan100% (1)
- Analysis Physiological IndicatorsDocument8 pagesAnalysis Physiological IndicatorsTatadarz Auxtero Lagria100% (1)
- The Role of Nurses in Diabetes Care and EducationDocument16 pagesThe Role of Nurses in Diabetes Care and EducationMakanjuola Osuolale JohnNo ratings yet
- Neuropati DMDocument30 pagesNeuropati DMAnisa PutriNo ratings yet
- CASP Qualitative Appraisal Checklist 14oct10Document12 pagesCASP Qualitative Appraisal Checklist 14oct10Agil SulistyonoNo ratings yet
- ANS RPN Integrated Post Test I A PDFDocument25 pagesANS RPN Integrated Post Test I A PDFdaljit chahalNo ratings yet
- 12 30 11 AADE Insulin WhitePaper PrintDocument17 pages12 30 11 AADE Insulin WhitePaper PrintMiguel Angel Fonseca RiveraNo ratings yet
- Endocrine System DiseasesDocument87 pagesEndocrine System DiseasesFahmiArifMuhammadNo ratings yet
- ISPAD Clinical Practice Consensus Guidelines 2018: Diabetic Ketoacidosis and The Hyperglycemic Hyperosmolar StateDocument23 pagesISPAD Clinical Practice Consensus Guidelines 2018: Diabetic Ketoacidosis and The Hyperglycemic Hyperosmolar StateJulietPérezNo ratings yet
- Insulin AdministrationDocument8 pagesInsulin AdministrationskybluealiNo ratings yet
- Non-Modifiable Risk Factors AreDocument10 pagesNon-Modifiable Risk Factors ArenurNo ratings yet
- Role of Family Support in African Americans with Type 2 DiabetesDocument6 pagesRole of Family Support in African Americans with Type 2 Diabetessamiran212No ratings yet
- Diabetes in The UK 2010Document21 pagesDiabetes in The UK 2010jrjsdNo ratings yet
- List of Items For A 24 HR PharmacyDocument3 pagesList of Items For A 24 HR PharmacyasgbalajiNo ratings yet
- Anatomy of The Endocrine System IIDocument129 pagesAnatomy of The Endocrine System IIShauie CayabyabNo ratings yet
- Classification Pathophysiology Diagnosis of DMDocument9 pagesClassification Pathophysiology Diagnosis of DMjohn haider gamolNo ratings yet
- Ketoacidosis A Rare Complication of Fibrocalculous Pancreatic Diabetes Ketoacidosis A Rare Complication of Fibrocalculous Pancreatic DiabetesDocument4 pagesKetoacidosis A Rare Complication of Fibrocalculous Pancreatic Diabetes Ketoacidosis A Rare Complication of Fibrocalculous Pancreatic DiabetesChintia Meliana Kathy SiraitNo ratings yet
- Urine AnalysisDocument33 pagesUrine AnalysisajaysomNo ratings yet
- Job Satisfaction Among Public Health Workers in Central Province Sri LankaDocument23 pagesJob Satisfaction Among Public Health Workers in Central Province Sri LankaGlobal Research and Development ServicesNo ratings yet
- Approved IFCC Recommendation On Reporting Results For Blood GlucoseDocument4 pagesApproved IFCC Recommendation On Reporting Results For Blood GlucosePham PhongNo ratings yet