You might also like
- Selective Serotonin Re-Uptake Inhibitors: in Child and Adolescent DepressionDocument6 pagesSelective Serotonin Re-Uptake Inhibitors: in Child and Adolescent DepressionLong HuynhNo ratings yet
- RozexDocument13 pagesRozexLong HuynhNo ratings yet
- Nurses and Midwives - Key Legislative RequirementsDocument7 pagesNurses and Midwives - Key Legislative RequirementsLong HuynhNo ratings yet
- Expert Commentary On Chronic OpioidsDocument5 pagesExpert Commentary On Chronic OpioidsLong HuynhNo ratings yet
- ConnectDocument2 pagesConnectLong HuynhNo ratings yet
- ConnectDocument3 pagesConnectLong HuynhNo ratings yet
- Bomb Defusal ManualDocument23 pagesBomb Defusal ManualcontactzumorioNo ratings yet
- Psychometric Success Abstract Reasoning - Practice Test 1Document13 pagesPsychometric Success Abstract Reasoning - Practice Test 1Ambrose Zaffar75% (16)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- A-Plus Early Criticalcare Brochure Full 20130529 FinalDocument18 pagesA-Plus Early Criticalcare Brochure Full 20130529 Finalnusthe2745No ratings yet
- PdrugDocument406 pagesPdrugAnonymous y3TIOwX8No ratings yet
- Science UnsolDocument31 pagesScience UnsolAmaan KhanNo ratings yet
- A Successful Occupational Health Nurse-Driven Health Promotion Program To Support Corporate SustainabilityDocument8 pagesA Successful Occupational Health Nurse-Driven Health Promotion Program To Support Corporate SustainabilitysriNo ratings yet
- The Unseen Side of Pregnancy: Non-Communicable Diseases and Maternal HealthDocument28 pagesThe Unseen Side of Pregnancy: Non-Communicable Diseases and Maternal HealthThe Wilson Center100% (2)
- Tensoval Comfort Classic ManualDocument2 pagesTensoval Comfort Classic Manualpocopepe2023No ratings yet
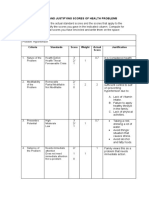
- C.2 Computing and Justifying Score of Health ProblemsDocument3 pagesC.2 Computing and Justifying Score of Health ProblemsHannah Angelu Cabading100% (1)
- 41 How To Cure DiseaseDocument60 pages41 How To Cure DiseaseEdie M Murgia50% (2)
- PamphletDocument2 pagesPamphletapi-25931970033% (3)
- CPG Hypertension PDFDocument77 pagesCPG Hypertension PDFvetina86% (7)
- (Journal) AN INNER QUALITY APPROACH TO REDUCINGDocument9 pages(Journal) AN INNER QUALITY APPROACH TO REDUCINGMery SanavieNo ratings yet
- Nursing Care PlanDocument2 pagesNursing Care PlanGwyneth SantiagoNo ratings yet
- Acute Glomerulonephriti S: Group 3Document25 pagesAcute Glomerulonephriti S: Group 3AradhanaRamchandaniNo ratings yet
- Treadmill Stress Test InstructionsDocument1 pageTreadmill Stress Test InstructionsMaria EdelNo ratings yet
- Management For HypertensionDocument8 pagesManagement For HypertensionSugimoto Karla Erika100% (1)
- Benefits and Drawbacks of Tele MedicineDocument11 pagesBenefits and Drawbacks of Tele MedicinessriraghavNo ratings yet
- Antenatal ExaminationDocument5 pagesAntenatal ExaminationAnuradha MauryaNo ratings yet
- Bates Chapter 4 Flashcards - QuizletDocument8 pagesBates Chapter 4 Flashcards - Quizletaznknight323No ratings yet
- Hipertensi 2021Document121 pagesHipertensi 2021puskesmas kasihan 1No ratings yet
- Yang Sheng 0211Document55 pagesYang Sheng 0211Redbaron88No ratings yet
- Obstetrics OBDocument65 pagesObstetrics OBVicviclookTheking100% (1)
- 6. Пульс, давлениеDocument3 pages6. Пульс, давлениеHurryNo ratings yet
- Massage Therapy EffectsDocument12 pagesMassage Therapy EffectsEkalevi FahlepieNo ratings yet
- Mind-Body Medicine - University of Maryland Medical CenterDocument17 pagesMind-Body Medicine - University of Maryland Medical Centerjle_dlNo ratings yet
- WelfareDocument23 pagesWelfareUmar BajwaNo ratings yet
- Practice Guidelines: High Blood Pressure: ACC/AHA Releases Updated GuidelineDocument3 pagesPractice Guidelines: High Blood Pressure: ACC/AHA Releases Updated GuidelineIris N MNo ratings yet
- HypertensionDocument23 pagesHypertensionrey magsayoNo ratings yet
- Managing Stress at Optimum Level For Superior Productivity: by Prof RN Krishnia Director-CTLD (TMU)Document23 pagesManaging Stress at Optimum Level For Superior Productivity: by Prof RN Krishnia Director-CTLD (TMU)Saransh GoelNo ratings yet
- Ethnobotanical Study of Acalypha Wilkesiana (Euphorbiaceae), A Plant Used in The Treatment of Arterial Hypertension in Oyem in Northern GabonDocument6 pagesEthnobotanical Study of Acalypha Wilkesiana (Euphorbiaceae), A Plant Used in The Treatment of Arterial Hypertension in Oyem in Northern GabonOpenaccess Research paperNo ratings yet
- Preclinical and Pain ContorolDocument57 pagesPreclinical and Pain ContorolEmad AlryashiNo ratings yet