You might also like
- Health Initiatives RFP: Keep New York Covered (KNYC)Document11 pagesHealth Initiatives RFP: Keep New York Covered (KNYC)Community Service Society of New YorkNo ratings yet
- CSS Testimony: Joint Legislative Session On HospitalsDocument12 pagesCSS Testimony: Joint Legislative Session On HospitalsCommunity Service Society of New YorkNo ratings yet
- How New Yorkers Feel About Affordability and Healthcare ReformDocument25 pagesHow New Yorkers Feel About Affordability and Healthcare ReformCommunity Service Society of New YorkNo ratings yet
- Testimony: City Council Hearing On Hospital Costs and Access To Care, 10/15/2021Document7 pagesTestimony: City Council Hearing On Hospital Costs and Access To Care, 10/15/2021Community Service Society of New YorkNo ratings yet
- Health Initiatives RFP: Uninsured Outreach Partners in Central and Western New YorkDocument13 pagesHealth Initiatives RFP: Uninsured Outreach Partners in Central and Western New YorkCommunity Service Society of New YorkNo ratings yet
- HCFANY Budget TestimonyDocument10 pagesHCFANY Budget TestimonyCommunity Service Society of New YorkNo ratings yet
- COVID-19 Financial Tips April 2021Document11 pagesCOVID-19 Financial Tips April 2021Community Service Society of New YorkNo ratings yet
- COVID-19 Financial Tips June 2020Document9 pagesCOVID-19 Financial Tips June 2020Community Service Society of New YorkNo ratings yet
- New York Housing Fact Sheet - Senate (Non NYC)Document38 pagesNew York Housing Fact Sheet - Senate (Non NYC)Community Service Society of New YorkNo ratings yet
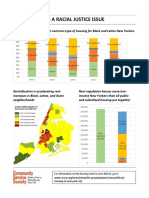
- Rent Justice As Racial JusticeDocument2 pagesRent Justice As Racial JusticeCommunity Service Society of New YorkNo ratings yet
- Patient Medical Debt Protection Act One PagerDocument1 pagePatient Medical Debt Protection Act One PagerCommunity Service Society of New YorkNo ratings yet
- COVID-19 Financial TipsDocument5 pagesCOVID-19 Financial TipsCommunity Service Society of New York100% (1)
- New York Housing Fact Sheet - Assembly (Non NYC)Document85 pagesNew York Housing Fact Sheet - Assembly (Non NYC)Community Service Society of New YorkNo ratings yet
- New York Housing Fact Sheet - NYC SenateDocument25 pagesNew York Housing Fact Sheet - NYC SenateCommunity Service Society of New YorkNo ratings yet
- Making College More Affordable For New Yorkers Who Need The Most SupportDocument17 pagesMaking College More Affordable For New Yorkers Who Need The Most SupportCommunity Service Society of New YorkNo ratings yet
- #FairFares Letter To MayorDocument2 pages#FairFares Letter To MayorDavid MeyerNo ratings yet
- Making College More Affordable For New Yorkers Who Need The Most Support - Unheard Third ChartsDocument7 pagesMaking College More Affordable For New Yorkers Who Need The Most Support - Unheard Third ChartsCommunity Service Society of New YorkNo ratings yet
- New York Housing Fact Sheet - NYC AssemblyDocument66 pagesNew York Housing Fact Sheet - NYC AssemblyCommunity Service Society of New YorkNo ratings yet
- Health Equity - Panel On Accessing Health Equity in New York City (Program)Document4 pagesHealth Equity - Panel On Accessing Health Equity in New York City (Program)Community Service Society of New YorkNo ratings yet
- Open Letter To Mayor de Blasio From Progressive LeadersDocument2 pagesOpen Letter To Mayor de Blasio From Progressive LeadersCommunity Service Society of New YorkNo ratings yet
- Health Professionals in Support of Paid Family LeaveDocument3 pagesHealth Professionals in Support of Paid Family LeaveCommunity Service Society of New YorkNo ratings yet
- Community Service Society's Role in Passing Paid Faimly Leave in New York.Document29 pagesCommunity Service Society's Role in Passing Paid Faimly Leave in New York.Community Service Society of New YorkNo ratings yet
- Community Service Society's Role in Passing Paid Family Leave in New York State.Document29 pagesCommunity Service Society's Role in Passing Paid Family Leave in New York State.Community Service Society of New YorkNo ratings yet
- NYC Alliance To Preserve Public Housing: October 2013 Letter To Chairman Rhea and Mayor BloombergDocument3 pagesNYC Alliance To Preserve Public Housing: October 2013 Letter To Chairman Rhea and Mayor BloombergCommunity Service Society of New YorkNo ratings yet
- Timeline: A Legacy of HopeDocument6 pagesTimeline: A Legacy of HopeCommunity Service Society of New York100% (1)
- New Yorkers Weigh in On Top Priorities For The New MayorDocument1 pageNew Yorkers Weigh in On Top Priorities For The New MayorCommunity Service Society of New YorkNo ratings yet
- NYC Alliance To Preserve Public Housing: Position On NYCHA's 2014 Annual PlanDocument10 pagesNYC Alliance To Preserve Public Housing: Position On NYCHA's 2014 Annual PlanCommunity Service Society of New YorkNo ratings yet
- CSS Center For Benefits & Services (CBS) One PagerDocument2 pagesCSS Center For Benefits & Services (CBS) One PagerCommunity Service Society of New YorkNo ratings yet
- PH Css Test Nycha Plan 610Document1 pagePH Css Test Nycha Plan 610Community Service Society of New YorkNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- SPC SoludoxDocument19 pagesSPC SoludoxMihai BirsaNo ratings yet
- Feed MixDocument4 pagesFeed MixTony1248No ratings yet
- Krok 2 Paper 4Document6 pagesKrok 2 Paper 4berdaderagaNo ratings yet
- Substance AbuseDocument3 pagesSubstance AbuseLuke VelasquezNo ratings yet
- NCP Ineffective Cerebral Tissue PerfusionDocument2 pagesNCP Ineffective Cerebral Tissue PerfusionAngelo ︻╦̵̵͇̿̿̿̿╤── Bulacan50% (6)
- Guillian-Barr e Syndrome - A Case StudyDocument11 pagesGuillian-Barr e Syndrome - A Case StudyHecan ComeNo ratings yet
- Infrastructure Requirement For B.Pharma & D. PharmaDocument2 pagesInfrastructure Requirement For B.Pharma & D. Pharmaanon_968573480No ratings yet
- GIT Conditions - StudentsDocument57 pagesGIT Conditions - StudentsShamal KoyeNo ratings yet
- NP2 Nursing Board Exam June 2008 Answer KeyDocument14 pagesNP2 Nursing Board Exam June 2008 Answer KeyBettina SanchezNo ratings yet
- ISO Grid Total BacterialDocument1 pageISO Grid Total Bacterialapi-3697331No ratings yet
- Case PresentationDocument82 pagesCase PresentationChadi Alraies100% (8)
- Medical Device Quality Systems Manual: A Small Entity Compliance GuideDocument468 pagesMedical Device Quality Systems Manual: A Small Entity Compliance GuideScott BeachNo ratings yet
- Pulse Oximeters Working PrincipleDocument2 pagesPulse Oximeters Working PrinciplealbertpatelusaNo ratings yet
- Pilates PaperDocument24 pagesPilates PaperSamantha SouzaNo ratings yet
- Dermocosmetic Care For RosaceaDocument16 pagesDermocosmetic Care For Rosaceariki fazar rahmaditaNo ratings yet
- MCAT SecretsDocument32 pagesMCAT SecretsTunde Ipaye100% (2)
- FDA - 162nd Meeting of The Vaccines and Related Biological ProductsDocument2 pagesFDA - 162nd Meeting of The Vaccines and Related Biological ProductsDavid CaplanNo ratings yet
- Foundations of Respiratory Medicine (2018) PDFDocument375 pagesFoundations of Respiratory Medicine (2018) PDFCristinaLucanNo ratings yet
- A Transition Program To Help Student-Athletes Move On To Lifetime Physical ActivityDocument12 pagesA Transition Program To Help Student-Athletes Move On To Lifetime Physical ActivityRaul Dario Pimentel GonzalezNo ratings yet
- Human Biology: Edexcel IGCSEDocument28 pagesHuman Biology: Edexcel IGCSEmuhajireenNo ratings yet
- ADHD: Clinical Practice Guideline For The Diagnosis, Evaluation, and TreatmentDocument18 pagesADHD: Clinical Practice Guideline For The Diagnosis, Evaluation, and TreatmentBen CulpepperNo ratings yet
- S1 Revision by Hania KhanDocument87 pagesS1 Revision by Hania KhanZoha AzizNo ratings yet
- RRL FinalDocument19 pagesRRL FinalGerald John PazNo ratings yet
- Sun Salutations Yoga Lesson PlanDocument8 pagesSun Salutations Yoga Lesson PlanErica Harris100% (1)
- TRIAZOLAMDocument4 pagesTRIAZOLAMEzequiel RosalesNo ratings yet
- "Breakfast Like A King, Lunch Like A Prince and Dinner Like A PauperDocument10 pages"Breakfast Like A King, Lunch Like A Prince and Dinner Like A Pauperதுர்காதேவிNo ratings yet
- 0.9% Sodium Chloride Injection, USP: Prescribing InformationDocument8 pages0.9% Sodium Chloride Injection, USP: Prescribing InformationarinNo ratings yet
- Human Kinetics Web Resources PDFDocument4 pagesHuman Kinetics Web Resources PDFyou waggaNo ratings yet
- Checklist For Iv Cannulation ProcedureDocument5 pagesChecklist For Iv Cannulation ProcedureMark Nel NuñezNo ratings yet
- The Effect of Physical Activity On Primary Dysmenorrhea of Female University StudentsDocument8 pagesThe Effect of Physical Activity On Primary Dysmenorrhea of Female University Studentssekar ayuNo ratings yet