You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Vedic Astrology OverviewDocument1 pageVedic Astrology Overviewhuman999100% (8)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Development of The FaceDocument76 pagesDevelopment of The Facedr parveen bathla100% (1)
- Vital Signs Reference Chart - 1Document1 pageVital Signs Reference Chart - 1l10n_assNo ratings yet
- Lubchenco Curve PDFDocument1 pageLubchenco Curve PDFWarren Lie25% (4)
- Surface Roughness Measurement - MitutoyoDocument2 pagesSurface Roughness Measurement - MitutoyoSelvaraj BalasundramNo ratings yet
- Schneider Power Supply PhaseoDocument26 pagesSchneider Power Supply PhaseoScott EnnisNo ratings yet
- Manual de Uso Ecografo GE Logiq e PDFDocument192 pagesManual de Uso Ecografo GE Logiq e PDFDaniel CortesNo ratings yet
- Hart Transmitter Calibration: Application NoteDocument8 pagesHart Transmitter Calibration: Application NoteThulasi Raman KowsiganNo ratings yet
- Specimen 1 ValuationDocument17 pagesSpecimen 1 ValuationLight BearerNo ratings yet
- Analytical Methods To Measure The Constants of Fats and OilsDocument5 pagesAnalytical Methods To Measure The Constants of Fats and OilsPenicillium Notatum67% (3)
- Toaz - Info Chemtech Reviewer PRDocument1 pageToaz - Info Chemtech Reviewer PRchristy janioNo ratings yet
- Callen2009 Clinically Relevant InformationDocument4 pagesCallen2009 Clinically Relevant Informationl10n_assNo ratings yet
- BMI Chart for Boys Ages 5-19Document1 pageBMI Chart for Boys Ages 5-19Justitia LantuNo ratings yet
- Beverly J. McCabe, Eric H. Frankel, Jonathan J. Wolfe Handbook of Food-Drug InteractionsDocument1 pageBeverly J. McCabe, Eric H. Frankel, Jonathan J. Wolfe Handbook of Food-Drug Interactionsl10n_assNo ratings yet
- Classification of Cutaneous LupusDocument5 pagesClassification of Cutaneous Lupusl10n_assNo ratings yet
- TABLE Boys 3mo To 5yr TRICEPSage PercentileDocument2 pagesTABLE Boys 3mo To 5yr TRICEPSage Percentilel10n_assNo ratings yet
- Jurnal Kriteria Baru SleDocument10 pagesJurnal Kriteria Baru SleDr Edi HidayatNo ratings yet
- Callen2004 Update On The Management of Cutaneous Lupus ErythematosusDocument6 pagesCallen2004 Update On The Management of Cutaneous Lupus Erythematosusl10n_assNo ratings yet
- Boeck Ler 2009Document5 pagesBoeck Ler 2009l10n_assNo ratings yet
- Z Score BMI 5-19yearsold Label GirlDocument1 pageZ Score BMI 5-19yearsold Label GirlVienny Widhyanti RosaryaNo ratings yet
- F E T C: Luid AND Lectrolyte Herapy IN HildrenDocument12 pagesF E T C: Luid AND Lectrolyte Herapy IN HildrenHartantoRezaGazaliNo ratings yet
- Temperature MeasurementDocument5 pagesTemperature Measurementl10n_ass100% (1)
- NPPA040112 DecisiontreeDocument1 pageNPPA040112 Decisiontreel10n_assNo ratings yet
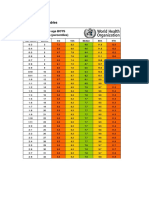
- Weight gain by birth weight and age groups for boysDocument1 pageWeight gain by birth weight and age groups for boysl10n_assNo ratings yet
- Bmi For Age Z-ScoreDocument1 pageBmi For Age Z-ScoreTisha Patricia OedoyNo ratings yet
- Bmifa Boys Z 5 19 LabelsDocument1 pageBmifa Boys Z 5 19 LabelssufigueiraNo ratings yet
- GCS PDFDocument1 pageGCS PDFFrincia100% (1)
- CSFDocument1 pageCSFl10n_assNo ratings yet
- PDFDocument1 pagePDFl10n_assNo ratings yet
- CHT Acfa Boys Z 3 5Document1 pageCHT Acfa Boys Z 3 5Rivadin NurwanNo ratings yet
- PDFDocument1 pagePDFl10n_assNo ratings yet
- CSFDocument1 pageCSFl10n_assNo ratings yet
- Dahlin2005 The Ketogenic Diet Influences The Levels of Excitatory and Inhibitory Amino Acids in The CSF in Children With Refractory EpilepsyDocument11 pagesDahlin2005 The Ketogenic Diet Influences The Levels of Excitatory and Inhibitory Amino Acids in The CSF in Children With Refractory Epilepsyl10n_assNo ratings yet
- Cunnane2002 Potential Role of Polyunsaturates in Seizure Protection Achieved With The Ketogenic DietDocument5 pagesCunnane2002 Potential Role of Polyunsaturates in Seizure Protection Achieved With The Ketogenic Dietl10n_assNo ratings yet
- Cross2013 New Research With Diets and EpilepsyDocument6 pagesCross2013 New Research With Diets and Epilepsyl10n_assNo ratings yet
- Brodie2005 Diagnosing and Predicting Refractory EpilepsyDocument4 pagesBrodie2005 Diagnosing and Predicting Refractory Epilepsyl10n_assNo ratings yet
- Best2000 Cardiac Complications in Pediatric Patients On The Ketogenic DietDocument3 pagesBest2000 Cardiac Complications in Pediatric Patients On The Ketogenic Dietl10n_assNo ratings yet
- Bough2007 Anticonvulsant Mechanisms of The Ketogenic DietDocument16 pagesBough2007 Anticonvulsant Mechanisms of The Ketogenic Dietl10n_assNo ratings yet
- ParikalpDocument43 pagesParikalpManish JaiswalNo ratings yet
- Operational Transconductance Amplifier ThesisDocument6 pagesOperational Transconductance Amplifier ThesislaurahallportlandNo ratings yet
- Student Pilot GuideDocument13 pagesStudent Pilot GuideAŞKIN FIRATNo ratings yet
- MC BreakdownDocument5 pagesMC BreakdownThane SnymanNo ratings yet
- DOCUMENT guides the way with VLB-44 LED Marine BeaconDocument4 pagesDOCUMENT guides the way with VLB-44 LED Marine BeaconbenNo ratings yet
- 3-Ph Induction MotorDocument246 pages3-Ph Induction MotorAn00pgadzillaNo ratings yet
- 43-101 Technical Report Quimsacocha, February 2009Document187 pages43-101 Technical Report Quimsacocha, February 2009Marco Vinicio SotoNo ratings yet
- Motherboards Tuf z270 Mark 2Document70 pagesMotherboards Tuf z270 Mark 2Jonah HexNo ratings yet
- ElectrochemistryDocument24 pagesElectrochemistryZainul AbedeenNo ratings yet
- Unchained MelodeeDocument93 pagesUnchained MelodeeRafael Cornholio RodriguezNo ratings yet
- Nordtest Method NT Fire 049Document16 pagesNordtest Method NT Fire 049mail2021No ratings yet
- Masterbrand Guidelines - September 2012: Confidential - For Internal Use OnlyDocument35 pagesMasterbrand Guidelines - September 2012: Confidential - For Internal Use OnlyDemerson CamposNo ratings yet
- Resultados de La Web: GDDS - Traducción Al Español - Ejemplos Inglés - Reverso ..Document3 pagesResultados de La Web: GDDS - Traducción Al Español - Ejemplos Inglés - Reverso ..Jo PaterninaNo ratings yet
- Personal Care Na Hair GuideDocument8 pagesPersonal Care Na Hair GuideIsabellaNo ratings yet
- Discrete Variable Probability Distribution FunctionsDocument47 pagesDiscrete Variable Probability Distribution FunctionsJanine CayabyabNo ratings yet
- Mast Bending Stress Calculation: Antenna 1Document6 pagesMast Bending Stress Calculation: Antenna 1Vinay KumarNo ratings yet
- WIP CaseStudyDocument3 pagesWIP CaseStudypaul porrasNo ratings yet
- Pitfalls of HIV Infection - Dr. Rizqi Amalia, Sp.ADocument46 pagesPitfalls of HIV Infection - Dr. Rizqi Amalia, Sp.AandreknhNo ratings yet
- 2017 Scoring Materials Math g6Document119 pages2017 Scoring Materials Math g6KRANo ratings yet
- Sing 2Document64 pagesSing 2WindsurfingFinnNo ratings yet
- 5 - Flight Recorder - OcrDocument19 pages5 - Flight Recorder - OcrtmhoangvnaNo ratings yet