You might also like
- SuctioningDocument31 pagesSuctioningmelanie silvaNo ratings yet
- Tracheostomy Care: Maintaining Airway PatencyDocument4 pagesTracheostomy Care: Maintaining Airway PatencyZar Ybañez MabanagNo ratings yet
- Tracheostomy CareDocument3 pagesTracheostomy CareKate Chavez100% (1)
- 8 Irrigating A ColostomyDocument5 pages8 Irrigating A ColostomyAnn Jalover PerezNo ratings yet
- Clinical Guidelines (Nursing) - Indwelling Urinary Catheter - Insertion and Ongoing CareDocument8 pagesClinical Guidelines (Nursing) - Indwelling Urinary Catheter - Insertion and Ongoing CareLeeNo ratings yet
- ThoracostomyDocument2 pagesThoracostomyJanelle MarceraNo ratings yet
- Colostomy CareDocument6 pagesColostomy CareLoren Sales ReyesNo ratings yet
- Procedure - Gastric LavageDocument2 pagesProcedure - Gastric LavageJose Paul RaderNo ratings yet
- Nebu&CPTDocument32 pagesNebu&CPTAbigail Bantayan100% (1)
- CVP - Nursing Performance ChecklistDocument3 pagesCVP - Nursing Performance ChecklistJoy Jarin75% (4)
- Nasal PolypsDocument20 pagesNasal PolypsPauleenNo ratings yet
- Chest Tube ThoracostomyDocument6 pagesChest Tube ThoracostomyRhea Lyn LamosteNo ratings yet
- Complications of IV TherapyDocument16 pagesComplications of IV TherapyFayeTolentinoNo ratings yet
- GIT Checklist With RationaleDocument5 pagesGIT Checklist With RationaleTeal OtterNo ratings yet
- Ostomy Care: Learning Manual DescriptionDocument12 pagesOstomy Care: Learning Manual DescriptionRenea Joy ArruejoNo ratings yet
- Legaspi - Preparing Medication From A Vial ChecklistDocument4 pagesLegaspi - Preparing Medication From A Vial ChecklistJason LumayaNo ratings yet
- Nasogastric Tube Feeding GuideDocument74 pagesNasogastric Tube Feeding GuideGoddy Manzano100% (1)
- Skin Grafting Surgical NursingDocument21 pagesSkin Grafting Surgical NursingHEMMA100% (1)
- NAIL AND FOOT CARE ROUTINEDocument5 pagesNAIL AND FOOT CARE ROUTINELexie KepnerNo ratings yet
- Administering Intradermal InjectionsDocument3 pagesAdministering Intradermal InjectionsKrisyll Meah Torred RamalNo ratings yet
- Tracheostomy Care and ManagementDocument63 pagesTracheostomy Care and ManagementAyesha FayyazNo ratings yet
- PATENTE - Worksheet - Nasogastric Tube Insertion, Feeding, and RemovalDocument11 pagesPATENTE - Worksheet - Nasogastric Tube Insertion, Feeding, and RemovalSelwynVillamorPatenteNo ratings yet
- Central Venous Pressure MonitoringDocument2 pagesCentral Venous Pressure MonitoringpauchanmnlNo ratings yet
- About Critical Care NursingDocument7 pagesAbout Critical Care NursingaivynNo ratings yet
- Pleural Fluid Analysis: How The Test Is PerformedDocument4 pagesPleural Fluid Analysis: How The Test Is PerformedKevin LlorenteNo ratings yet
- Paroxysmal Nocturnal Hemoglobinuria Case StudyDocument87 pagesParoxysmal Nocturnal Hemoglobinuria Case Studyrachael100% (4)
- Urine Specimen CollectionDocument3 pagesUrine Specimen Collectionyota_ahlyNo ratings yet
- Lesson 1 POST TEST Maternal FrameworkDocument1 pageLesson 1 POST TEST Maternal FrameworkAnnalisa TellesNo ratings yet
- CHN 2 JournalDocument2 pagesCHN 2 Journalinah krizia lagueNo ratings yet
- Nasopharyngeal Suctioning GuideDocument6 pagesNasopharyngeal Suctioning GuideJmarie Brillantes PopiocoNo ratings yet
- Nasogastric Tube Feeding GuideDocument20 pagesNasogastric Tube Feeding GuideKrishna Sonu SoniNo ratings yet
- Nursing Theory: Asthma (Presentation)Document13 pagesNursing Theory: Asthma (Presentation)vinda astri permatasari100% (1)
- Mabini Colleges' Mission and Vision for Transforming StudentsDocument12 pagesMabini Colleges' Mission and Vision for Transforming StudentsKaren Kate AblesNo ratings yet
- PEG Feeding Procedure GuideDocument3 pagesPEG Feeding Procedure GuideAlyzza Dagoy100% (1)
- Tonsillitis, Tonsillectomy, and Adenoidectomy: Professor Sameer Bafaqeeh, M.DDocument50 pagesTonsillitis, Tonsillectomy, and Adenoidectomy: Professor Sameer Bafaqeeh, M.DMrprads5No ratings yet
- Assessing The Respiratory System (Thorax & Lungs)Document3 pagesAssessing The Respiratory System (Thorax & Lungs)JENNA ELOISA UYNo ratings yet
- HernioplastyDocument6 pagesHernioplastyCherry Delos ReyesNo ratings yet
- Nursing Care for Patients with ColostomyDocument26 pagesNursing Care for Patients with ColostomyKyle Ü D. CunanersNo ratings yet
- Nasogastric Tube InsertionDocument3 pagesNasogastric Tube Insertionmarie100% (5)
- Reteplase (MIRel)Document23 pagesReteplase (MIRel)Jhoann JamanilaNo ratings yet
- Schematic Diagram BA HAP HRDocument2 pagesSchematic Diagram BA HAP HRMika MinsalanNo ratings yet
- COPD - Chronic Obstructive Pulmonary DiseaseDocument30 pagesCOPD - Chronic Obstructive Pulmonary DiseaseAmila SirisingheNo ratings yet
- Tension Pneumothorax: Modifiable FactorsDocument3 pagesTension Pneumothorax: Modifiable FactorsJustin MaverickNo ratings yet
- TonsillectomyDocument6 pagesTonsillectomyBen David0% (1)
- Moira Mae B. Balite BSN 2A: Post Partum Care DefinitionDocument5 pagesMoira Mae B. Balite BSN 2A: Post Partum Care DefinitionMoiraMaeBeridoBaliteNo ratings yet
- NCM 116 ChecklistsDocument14 pagesNCM 116 Checklistsmark OrpillaNo ratings yet
- Nasogastric Tube Placement GuidelinesDocument17 pagesNasogastric Tube Placement Guidelinesdrsupriyagmc9507100% (1)
- Chapter IDocument22 pagesChapter Icoosa liquorsNo ratings yet
- Drug StudyDocument2 pagesDrug StudyJayran Bay-anNo ratings yet
- Appendicitis: Causes, Symptoms, Diagnosis and TreatmentDocument35 pagesAppendicitis: Causes, Symptoms, Diagnosis and TreatmentleighjagNo ratings yet
- Gallbladder Removal Procedure and RecoveryDocument6 pagesGallbladder Removal Procedure and RecoveryTom Bayubs-tucsNo ratings yet
- Urinary Catheterization Procedures With RationaleDocument10 pagesUrinary Catheterization Procedures With RationaleKaye NaigNo ratings yet
- Insulin Injection Technique GuideDocument23 pagesInsulin Injection Technique Guideimamori100% (1)
- Water Sealed DrainageDocument2 pagesWater Sealed DrainagefairwoodsNo ratings yet
- Perilite and Hot SitzDocument11 pagesPerilite and Hot SitzJyra Mae TaganasNo ratings yet
- NSO Gastric LavageDocument3 pagesNSO Gastric Lavagetry dokkNo ratings yet
- Skills (Tracheostomy Care)Document5 pagesSkills (Tracheostomy Care)kimtalaNo ratings yet
- Tracheostomy CareDocument25 pagesTracheostomy Caremelanie silvaNo ratings yet
- Tracheostomy CareDocument15 pagesTracheostomy CareZabeth ZabNo ratings yet
- Tracheostomy CareDocument15 pagesTracheostomy CareZabeth ZabNo ratings yet
- Introduction Brain Abcess Nursing ManagementDocument2 pagesIntroduction Brain Abcess Nursing ManagementCalimlim KimNo ratings yet
- Why Study A Masters in Surgical Nursing?Document5 pagesWhy Study A Masters in Surgical Nursing?Calimlim KimNo ratings yet
- How to open a password protected zip fileDocument2 pagesHow to open a password protected zip fileSumber UnduhNo ratings yet
- Sal But AmolDocument2 pagesSal But AmolCalimlim KimNo ratings yet
- NCPsDocument11 pagesNCPsCalimlim KimNo ratings yet
- NursingDocument4 pagesNursingCalimlim KimNo ratings yet
- Path o Physiology GastrroDocument1 pagePath o Physiology GastrroCalimlim KimNo ratings yet
- Bioethics Assignment 1Document2 pagesBioethics Assignment 1Calimlim KimNo ratings yet
- Understanding Breast DisordersDocument13 pagesUnderstanding Breast DisordersCalimlim KimNo ratings yet
- Bioethics Assignment 1Document2 pagesBioethics Assignment 1Calimlim KimNo ratings yet
- Prelim Bioethics Handouts.Document13 pagesPrelim Bioethics Handouts.Calimlim KimNo ratings yet
- Red Cross 143 Program 3Document23 pagesRed Cross 143 Program 3Calimlim KimNo ratings yet
- Chapter 18Document34 pagesChapter 18Calimlim KimNo ratings yet
- Effects of Social Media on Nurses' Work PerformanceDocument42 pagesEffects of Social Media on Nurses' Work PerformanceCalimlim Kim100% (1)
- The Importance of SanitationDocument3 pagesThe Importance of SanitationCalimlim KimNo ratings yet
- FINAL Discharge-PlanningDocument3 pagesFINAL Discharge-PlanningCalimlim KimNo ratings yet
- Pathophysiology CHF MineDocument2 pagesPathophysiology CHF MineCalimlim KimNo ratings yet
- Working Phase (Psych Nursing) Progress Report Process ReportingDocument5 pagesWorking Phase (Psych Nursing) Progress Report Process ReportingCalimlim KimNo ratings yet
- Lnu Case SlipDocument4 pagesLnu Case SlipCalimlim KimNo ratings yet
- Case SlipDocument4 pagesCase SlipCalimlim KimNo ratings yet
- Nursing Care Plan: Cues Nursing Diagnosis Analysis Goal and Objectives Interventions Rationale EvaluationDocument3 pagesNursing Care Plan: Cues Nursing Diagnosis Analysis Goal and Objectives Interventions Rationale EvaluationCalimlim KimNo ratings yet
- Philippine Anti CyberbullyingDocument4 pagesPhilippine Anti CyberbullyingCalimlim Kim100% (2)
- CSR AppDocument2 pagesCSR AppCalimlim KimNo ratings yet
- Case PresentationDocument55 pagesCase PresentationCalimlim KimNo ratings yet
- Late Onset Asthma & Cardiovascular Disease RisksDocument2 pagesLate Onset Asthma & Cardiovascular Disease RisksCalimlim KimNo ratings yet
- Laboratory Result SampleDocument2 pagesLaboratory Result SampleCalimlim KimNo ratings yet
- Case Slip DRDocument4 pagesCase Slip DRCalimlim KimNo ratings yet
- Dumping Syndrome 508Document8 pagesDumping Syndrome 508Calimlim KimNo ratings yet
- A Novel Mouse Model of High FlowDocument1 pageA Novel Mouse Model of High FlowCalimlim KimNo ratings yet
- Disturbed Sensory PerceptionDocument3 pagesDisturbed Sensory PerceptionCalimlim Kim100% (1)
- Respiratory and Circulatory Systems WorksheetDocument6 pagesRespiratory and Circulatory Systems WorksheetJaimeCrispinoNo ratings yet
- Medical Surgical (MS) Lecture Respiratory System: Alteration in OxygenationDocument44 pagesMedical Surgical (MS) Lecture Respiratory System: Alteration in OxygenationYman Gio BumanglagNo ratings yet
- The Different Types of Respiratory Diseases Prevalent in KenyaDocument9 pagesThe Different Types of Respiratory Diseases Prevalent in KenyaKimberlyNekesaNo ratings yet
- Enterobacteriaceae: Dr. BetsyDocument36 pagesEnterobacteriaceae: Dr. BetsySoham BanikNo ratings yet
- Study GuideDocument17 pagesStudy GuideKellie PacanowskiNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD)Document86 pagesChronic Obstructive Pulmonary Disease (COPD)physio43No ratings yet
- ANP1105 Final Exam Review - Respiratory, Lymphatic SystemsDocument4 pagesANP1105 Final Exam Review - Respiratory, Lymphatic SystemsVienna GilmoreNo ratings yet
- Bronchial AsthmaDocument34 pagesBronchial AsthmaFabb NelsonNo ratings yet
- Introduction - Case PresentationDocument16 pagesIntroduction - Case PresentationcherylNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument76 pagesChronic Obstructive Pulmonary DiseasedidinNo ratings yet
- Science 6: Let'S Work Together!Document26 pagesScience 6: Let'S Work Together!Xivaughn SebastianNo ratings yet
- Respiratory Functions OverviewDocument17 pagesRespiratory Functions OverviewMustak AhmedNo ratings yet
- Herbs-Sam CoffmanDocument9 pagesHerbs-Sam CoffmanSilambarasu Karuppiah0% (1)
- Medicinal Plants From Siddha System of Medicine Useful For Treating Respiratory DiseasesDocument11 pagesMedicinal Plants From Siddha System of Medicine Useful For Treating Respiratory DiseasessweetohmNo ratings yet
- Respi-Nclex QuestionsDocument160 pagesRespi-Nclex QuestionsSophia Rose Delos Santos100% (3)
- Report Respiratory SystemDocument6 pagesReport Respiratory SystemDan Dan Soi T100% (1)
- Makalah B. Inggris SputumDocument8 pagesMakalah B. Inggris SputumDian FaqihNo ratings yet
- Atelectasis EditedDocument40 pagesAtelectasis EditedAimee Gutierrez100% (1)
- Sample The Human Body Worksheets 1Document18 pagesSample The Human Body Worksheets 1Jan Erika AlmeronNo ratings yet
- The Microscopic Structure and Functions of the Respiratory SystemDocument67 pagesThe Microscopic Structure and Functions of the Respiratory SystemADE DWINATA SUSILO PUTRINo ratings yet
- Air Pollution Lect.1Document277 pagesAir Pollution Lect.1Nah Sr AdNo ratings yet
- Oxygen InsufficiencyDocument16 pagesOxygen Insufficiencydeolzf100% (1)
- Respiratory ExaminationDocument59 pagesRespiratory ExaminationNur Hamizah Md FuziNo ratings yet
- ITE NOTES (AutoRecovered)Document17 pagesITE NOTES (AutoRecovered)claravhvuNo ratings yet
- Complete Breathing and Exchange of GasesDocument20 pagesComplete Breathing and Exchange of GasesANo ratings yet
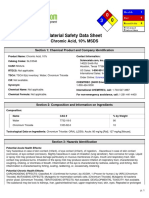
- MsdsDocument6 pagesMsdsRUFUSNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument9 pagesChronic Obstructive Pulmonary DiseaseKiara Denise TamayoNo ratings yet
- Anh 10 - de Xuat de Thi Va Dap An Thi DH 2016 - CVADocument18 pagesAnh 10 - de Xuat de Thi Va Dap An Thi DH 2016 - CVAEthan JonesNo ratings yet
- ParamyxoviridaeDocument27 pagesParamyxoviridaeFarrah BenoitNo ratings yet
- PneumoniaDocument17 pagesPneumoniajustin_saneNo ratings yet