You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- BothaDocument20 pagesBothaScott DonianNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Cooper JBLDocument25 pagesCooper JBLScott DonianNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Bullmore TRINJDocument25 pagesBullmore TRINJScott DonianNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Lion, The Wicked, and The Wonder of It All: Psalm 104 and The Playful GodDocument7 pagesThe Lion, The Wicked, and The Wonder of It All: Psalm 104 and The Playful GodScott DonianNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- XX BrueggemannDocument19 pagesXX BrueggemannScott DonianNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Proceedings of The International Conference The Proceedings of The International Conference On Creationism On CreationismDocument9 pagesThe Proceedings of The International Conference The Proceedings of The International Conference On Creationism On CreationismScott DonianNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- God's all-knowing presenceDocument22 pagesGod's all-knowing presenceScott DonianNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Adler JBQDocument5 pagesAdler JBQScott DonianNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- X Cook ZAWDocument19 pagesX Cook ZAWScott DonianNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Psalm 104: A Bodily Interpretation of Yahweh's History': J H. C D B R S U JDocument12 pagesPsalm 104: A Bodily Interpretation of Yahweh's History': J H. C D B R S U JScott DonianNo ratings yet
- Creation Sings To The Trinity: The Great Drama of The Hymn "Holy, Holy, Holy"Document5 pagesCreation Sings To The Trinity: The Great Drama of The Hymn "Holy, Holy, Holy"Scott DonianNo ratings yet
- Creation Sings To The Trinity: The Great Drama of The Hymn "Holy, Holy, Holy"Document5 pagesCreation Sings To The Trinity: The Great Drama of The Hymn "Holy, Holy, Holy"Scott DonianNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Waters of The Earth: An Exegetical Study of PSALM 104:1-9Document24 pagesThe Waters of The Earth: An Exegetical Study of PSALM 104:1-9Scott DonianNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unexpected Uni Erse: Emergence, Con Ergence, and The O Erview Effect"Document15 pagesThe Unexpected Uni Erse: Emergence, Con Ergence, and The O Erview Effect"Scott DonianNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Baptism of Jesus According To The Gospel of Mark: JETS SA/1 (March 1991) 43-57Document16 pagesThe Baptism of Jesus According To The Gospel of Mark: JETS SA/1 (March 1991) 43-57Scott DonianNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Jesus' Philosophy of Ministry: A Study of A Figure of Speech in Mark 1:38Document4 pagesJesus' Philosophy of Ministry: A Study of A Figure of Speech in Mark 1:38Scott DonianNo ratings yet
- Van OyenDocument6 pagesVan OyenScott DonianNo ratings yet
- Ffi-Pffiu$: Ffi Ilifu R,,:,,in L ,)Document9 pagesFfi-Pffiu$: Ffi Ilifu R,,:,,in L ,)Scott DonianNo ratings yet
- Mark 6:6b-30: Mission, The Baptist, and Failure: Francis J. Moloney, S.D.BDocument18 pagesMark 6:6b-30: Mission, The Baptist, and Failure: Francis J. Moloney, S.D.BScott DonianNo ratings yet
- "As One Having Authority" (Mark 1:22) : The Controversial Distinction of Jesus' TeachingDocument23 pages"As One Having Authority" (Mark 1:22) : The Controversial Distinction of Jesus' TeachingScott DonianNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- X Patterson JETS PDFDocument22 pagesX Patterson JETS PDFScott DonianNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- XX Kaltner JBLDocument5 pagesXX Kaltner JBLScott DonianNo ratings yet
- XX Smelik JSOTDocument8 pagesXX Smelik JSOTScott DonianNo ratings yet
- XX Brug WISLUTQDocument3 pagesXX Brug WISLUTQScott DonianNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Analysis of the textual variations between II Samuel 22 and Psalm 18Document21 pagesAnalysis of the textual variations between II Samuel 22 and Psalm 18Scott DonianNo ratings yet
- Sulzbach SJOTDocument25 pagesSulzbach SJOTScott DonianNo ratings yet
- XX Balentine JPRDocument7 pagesXX Balentine JPRScott DonianNo ratings yet
- Short Notes: ? As (The Anchor Bible, PsalmsDocument3 pagesShort Notes: ? As (The Anchor Bible, PsalmsScott DonianNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- X Coetzee OTEDocument21 pagesX Coetzee OTEScott DonianNo ratings yet
- X Kuntz JSOTDocument30 pagesX Kuntz JSOTScott DonianNo ratings yet
- Art Appreciation 3Document7 pagesArt Appreciation 3Asher SarcenoNo ratings yet
- Santrock3 PPT Ch01Document35 pagesSantrock3 PPT Ch01Syarafina Abdullah67% (3)
- Active View of ReadingDocument20 pagesActive View of ReadingiefabiandiazNo ratings yet
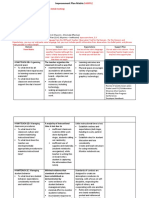
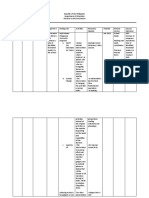
- Improvement Plan MatrixDocument3 pagesImprovement Plan MatrixJESSA MAE ORPILLANo ratings yet
- Knotion Writing GuideDocument20 pagesKnotion Writing GuideSandra Torres100% (1)
- Comparing Decimals 4th Grade LessonDocument5 pagesComparing Decimals 4th Grade Lessonapi-455810519No ratings yet
- Foreign Literatures: Deb, S., Strodl, E., & Sun, H. 2015)Document10 pagesForeign Literatures: Deb, S., Strodl, E., & Sun, H. 2015)Rose ann BulalacaoNo ratings yet
- Home Health ToolboxDocument32 pagesHome Health ToolboxFred TomNo ratings yet
- Psychoanalytic CriticismDocument20 pagesPsychoanalytic CriticismFakhirah Ab AzizNo ratings yet
- Subtracting with 10: A Detailed Lesson PlanDocument7 pagesSubtracting with 10: A Detailed Lesson PlanKathrine Faye OsallaNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 2.0 Training Needs Analysis (Tna) 2.1 Objectives of Training Needs AnalysisDocument16 pages2.0 Training Needs Analysis (Tna) 2.1 Objectives of Training Needs AnalysisNoor Azizah Binti JakariaNo ratings yet
- Computer: 01 Hour and A HalfDocument3 pagesComputer: 01 Hour and A HalfMohammedBaouaisseNo ratings yet
- ForceandmotionfrictionlessonplanDocument3 pagesForceandmotionfrictionlessonplanapi-272546079No ratings yet
- Mathematical Communication Ability and Curiosity Attitude Through Problem Based Learning and Cognitive Conflict Strategy Based On Academic Level: A Study in Number TheoryDocument17 pagesMathematical Communication Ability and Curiosity Attitude Through Problem Based Learning and Cognitive Conflict Strategy Based On Academic Level: A Study in Number TheoryGlobal Research and Development ServicesNo ratings yet
- Explaining The Placebo Effect: Aliefs, Beliefs, and ConditioningDocument33 pagesExplaining The Placebo Effect: Aliefs, Beliefs, and ConditioningDjayuzman No MagoNo ratings yet
- Lesson 4 With Review Powerpoint LANGUAGE ACQUISITIONDocument140 pagesLesson 4 With Review Powerpoint LANGUAGE ACQUISITIONGodwin Jerome ReyesNo ratings yet
- Ai Robocom: Mick G.D. Remmerswaal March 18, 2020Document11 pagesAi Robocom: Mick G.D. Remmerswaal March 18, 2020Mick RemmerswaalNo ratings yet
- Piaget, Jean 1980Document6 pagesPiaget, Jean 1980Dhian Gowinda Luh SafitriNo ratings yet
- Action PlanDocument3 pagesAction PlanIvy BarnacheaNo ratings yet
- Vygotsky’s Social Constructivist Theory of LearningDocument9 pagesVygotsky’s Social Constructivist Theory of LearningJascha KimNo ratings yet
- Prime Time 3 Work Book 78-138pgDocument60 pagesPrime Time 3 Work Book 78-138pgSalome SamushiaNo ratings yet
- STENIUS, Erik - Wittgenstein's Tractatus. A Critical Exposition of Its Main Lines of ThoughtsDocument250 pagesSTENIUS, Erik - Wittgenstein's Tractatus. A Critical Exposition of Its Main Lines of ThoughtsJuan ErlleNo ratings yet
- File 2 Answer Key A: Grammar, Vocabulary, and Pronunciation GrammarDocument6 pagesFile 2 Answer Key A: Grammar, Vocabulary, and Pronunciation GrammarZ ZorroNo ratings yet
- Finaal PPT EfcomDocument17 pagesFinaal PPT EfcomRolyn BonghanoyNo ratings yet
- Issue Emotion Why Do You Feel That Way? How Will You Deal With Positive/ Negative EmotionDocument2 pagesIssue Emotion Why Do You Feel That Way? How Will You Deal With Positive/ Negative Emotionjane gwapaNo ratings yet
- The Limits of Cladism - by David L. Hull Systematic Zoology, Vol. 28, No. 4 (Dec., 1979), Pp. 416-440.Document26 pagesThe Limits of Cladism - by David L. Hull Systematic Zoology, Vol. 28, No. 4 (Dec., 1979), Pp. 416-440.AbuAbdur-RazzaqAl-MisriNo ratings yet
- Early Maladaptive SchemasDocument7 pagesEarly Maladaptive Schemaskanny olojugbaNo ratings yet
- David's Day - Interactive Worksheet: Esl / Efl ResourcesDocument1 pageDavid's Day - Interactive Worksheet: Esl / Efl ResourcesIsabella Henao AmayaNo ratings yet
- Skema Bahasa Inggeris K1 & K2Document5 pagesSkema Bahasa Inggeris K1 & K2Naz JaafarNo ratings yet
- The Self-Objectification Scale - A New Measure For Assessing SelfDocument5 pagesThe Self-Objectification Scale - A New Measure For Assessing SelfManuel CerónNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)
- Techniques Exercises And Tricks For Memory ImprovementFrom EverandTechniques Exercises And Tricks For Memory ImprovementRating: 4.5 out of 5 stars4.5/5 (40)
- The Ultimate Guide To Memory Improvement TechniquesFrom EverandThe Ultimate Guide To Memory Improvement TechniquesRating: 5 out of 5 stars5/5 (34)
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeFrom EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeNo ratings yet
- The Happiness Trap: How to Stop Struggling and Start LivingFrom EverandThe Happiness Trap: How to Stop Struggling and Start LivingRating: 4 out of 5 stars4/5 (1)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsFrom EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsRating: 3.5 out of 5 stars3.5/5 (3)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)