You might also like
- Critical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeFrom EverandCritical Care for Anorexia Nervosa: The MARSIPAN Guidelines in PracticeNo ratings yet
- Current Clinical Strategies: Handbook of Psychiatric DrugsDocument72 pagesCurrent Clinical Strategies: Handbook of Psychiatric Drugsmike116No ratings yet
- Hypnotics Anxiolytics GuidelinesDocument28 pagesHypnotics Anxiolytics GuidelinesClarissa YudakusumaNo ratings yet
- PocketGuide FINAL6 PDFDocument2 pagesPocketGuide FINAL6 PDFSolomon Seth SallforsNo ratings yet
- Algorithm - Managing A COPD Exacerbation in Primary CareDocument1 pageAlgorithm - Managing A COPD Exacerbation in Primary Caremufidah mawaddahNo ratings yet
- Chest & Abdominal X-Ray Interpretation: LT Col NK Jain GD SPL (Radiology) MH JabalpurDocument116 pagesChest & Abdominal X-Ray Interpretation: LT Col NK Jain GD SPL (Radiology) MH JabalpurabolojeenNo ratings yet
- HCSW - Holistic Care and Assessment in Primary CareDocument1 pageHCSW - Holistic Care and Assessment in Primary CaregireeshsachinNo ratings yet
- Oral Pharmacologic Treatment of Type 2 Diabetes Mellitus: A Clinical Practice Guideline Update From The American College of PhysiciansDocument20 pagesOral Pharmacologic Treatment of Type 2 Diabetes Mellitus: A Clinical Practice Guideline Update From The American College of PhysiciansRoberto López MataNo ratings yet
- Intensive Nursing Practicum: SchizophreniaDocument44 pagesIntensive Nursing Practicum: SchizophreniaAngelicaNo ratings yet
- Diagnostic and Management Guidelines For Mental Disorders in Primary CareDocument98 pagesDiagnostic and Management Guidelines For Mental Disorders in Primary CareLa Safuan AzkarNo ratings yet
- Psycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsDocument29 pagesPsycho-Pharmacotherapy: Major Tranquilizers, D2 - Receptor Blockers and Anti - Schizophrenic DrugsPoonam RanaNo ratings yet
- CHT DMARDDocument3 pagesCHT DMARDkoolaberNo ratings yet
- Antipsychotic or Neuroleptic DrugsDocument12 pagesAntipsychotic or Neuroleptic Drugscamile buhanginNo ratings yet
- Dosage and Pharmacology of Antipsychotics - UpToDate ...Document4 pagesDosage and Pharmacology of Antipsychotics - UpToDate ...Dragutin PetrićNo ratings yet
- Asthma Clinical Care GuidelinesDocument17 pagesAsthma Clinical Care GuidelinesWalaa MoustafaNo ratings yet
- Extended Guideline Mental HealthDocument222 pagesExtended Guideline Mental Healthapi-26041148No ratings yet
- Eye ExaminationDocument23 pagesEye Examinationcynthia167No ratings yet
- Primary Care Antibiotic Guideline FINAL May 2015Document10 pagesPrimary Care Antibiotic Guideline FINAL May 2015Atta Muhammad MemonNo ratings yet
- Depression - Let's TalkDocument9 pagesDepression - Let's TalkThavam RatnaNo ratings yet
- Standard Treatment Guidelines and Essential Medicine List For Primary Health Care 7th Edition - 2020Document626 pagesStandard Treatment Guidelines and Essential Medicine List For Primary Health Care 7th Edition - 2020Finger TladiNo ratings yet
- Invega+Sustenna PiDocument18 pagesInvega+Sustenna PiMaal AbrarNo ratings yet
- Antiarrhythmic Medication Chart - EBM Consult v3Document2 pagesAntiarrhythmic Medication Chart - EBM Consult v3Linlin100% (1)
- Guidelines For The Management of Common Mental DisordersDocument95 pagesGuidelines For The Management of Common Mental DisordersAruna HarikrishnanNo ratings yet
- 2nd Edn ID MHFA Manual Sept 2012 SmallDocument125 pages2nd Edn ID MHFA Manual Sept 2012 SmallAnonymous Nvv1TaS7100% (1)
- Standard Treatment GuidelinesDocument5 pagesStandard Treatment Guidelinesbournvilleeater100% (1)
- Foot and Toe Nail Care GuidelinesDocument6 pagesFoot and Toe Nail Care GuidelineskyleNo ratings yet
- TramadolDocument3 pagesTramadolKaren Viviene Aberilla CincoNo ratings yet
- Northern Ireland Management of Infection Guidelines For Primary and Community Care 2016Document48 pagesNorthern Ireland Management of Infection Guidelines For Primary and Community Care 2016dreneavalentinstefanNo ratings yet
- Depression in Older Adults: A Treatable Medical ConditionDocument12 pagesDepression in Older Adults: A Treatable Medical ConditionJose Alonso Aguilar Valera100% (1)
- 1: Adhd: Scientific Name Dose CommentsDocument4 pages1: Adhd: Scientific Name Dose CommentsSadiq Abdo92No ratings yet
- Guidelines+ +Opioids+ChapterDocument16 pagesGuidelines+ +Opioids+ChapterRajinder Kumar BassanNo ratings yet
- Adult Headache GuidelinesDocument7 pagesAdult Headache Guidelinespallavi priyamNo ratings yet
- Preventive Care Guidelines 2016 PediatricDocument3 pagesPreventive Care Guidelines 2016 PediatricAnonymous ic2CDkFNo ratings yet
- Headache Chart PDFDocument3 pagesHeadache Chart PDFrajakoppulaNo ratings yet
- Primary Health Care Hand Outs For StudentsDocument35 pagesPrimary Health Care Hand Outs For StudentsGreggy VenturaNo ratings yet
- SchizopDocument43 pagesSchizopapi-548578435No ratings yet
- Cardiology Flash CardsDocument5 pagesCardiology Flash CardsRodrigo FonsecaNo ratings yet
- MMP Handy Chart October 2011 V2Document69 pagesMMP Handy Chart October 2011 V2Icha IchaNo ratings yet
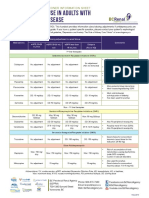
- Antidepressant Use in Adults With Chronic Kidney DiseaseDocument1 pageAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- Psychiatric Medication 2021Document15 pagesPsychiatric Medication 2021Gyanendra ChaudharyNo ratings yet
- ACLS AgorithmDocument55 pagesACLS AgorithmkpsuanNo ratings yet
- Guidelines For The Management of Alcohol Dependendence and Acute Withdrawal On General Psychiatry Wards May 2017Document10 pagesGuidelines For The Management of Alcohol Dependendence and Acute Withdrawal On General Psychiatry Wards May 2017renzo85rhNo ratings yet
- Outpatient MedicineDocument0 pagesOutpatient Medicineclaragustin_53768590No ratings yet
- Medication PrescribingDocument13 pagesMedication PrescribingadrianaNo ratings yet
- Dot Medical Exam BoerneDocument5 pagesDot Medical Exam BoernecdldocNo ratings yet
- Emergency Pediatric AidsDocument29 pagesEmergency Pediatric AidsRana SalemNo ratings yet
- Depression PP FVDocument62 pagesDepression PP FVSharmela Brijmohan100% (1)
- 6675 Final ExamDocument32 pages6675 Final ExamtroillerdrippyNo ratings yet
- AnxietyDocument5 pagesAnxietyJohn HolmesNo ratings yet
- Handy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Document3 pagesHandy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Mariya ZhekovaNo ratings yet
- ACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientDocument1 pageACLS Algorithm Pulse No Yes: Stable Patient Unstable Patient Stable PatientAhmed AlkhaqaniNo ratings yet
- Geriatric Giants - DR SeymourDocument108 pagesGeriatric Giants - DR SeymourSharon Mallia100% (1)
- Second-Generation Antipsychotics and Pregnancy ComplicationsDocument9 pagesSecond-Generation Antipsychotics and Pregnancy ComplicationsDian Oktaria SafitriNo ratings yet
- Final Coaching DrugsDocument8 pagesFinal Coaching DrugsSherlyn BesasNo ratings yet
- Essenc I Al TherapyDocument9 pagesEssenc I Al TherapyFabian Ramirez HincapiéNo ratings yet
- Anxiety and Depression in Tinnitus Sufferers PDFDocument8 pagesAnxiety and Depression in Tinnitus Sufferers PDFMayra WainsNo ratings yet
- Se Insulin Stability ChartDocument2 pagesSe Insulin Stability ChartWirmanNo ratings yet
- Primary Health Care WHO OverviewDocument16 pagesPrimary Health Care WHO OverviewlilaningNo ratings yet
- A Nurse PractitionerDocument4 pagesA Nurse PractitionerN.DanielaNo ratings yet
- The Five Major Religions: Social Studies OnlineDocument25 pagesThe Five Major Religions: Social Studies OnlineAllan DiasNo ratings yet
- Agitated PatientDocument45 pagesAgitated PatientAllan DiasNo ratings yet
- Body Dysmorphic DisorderDocument6 pagesBody Dysmorphic DisorderAllan DiasNo ratings yet
- Emergencias Psiquiatricas InglesDocument29 pagesEmergencias Psiquiatricas InglesAllan DiasNo ratings yet
- Hysterical PsychosisDocument13 pagesHysterical PsychosisAllan DiasNo ratings yet
- The Five Major Religions: Social Studies OnlineDocument25 pagesThe Five Major Religions: Social Studies OnlineAllan DiasNo ratings yet
- Treatment Options For InsomniaDocument10 pagesTreatment Options For InsomniaAllan DiasNo ratings yet
- TEPTDocument6 pagesTEPTAllan DiasNo ratings yet
- Andrew Moskovitz Psychotic Symptoms in Rape SurvivorsDocument20 pagesAndrew Moskovitz Psychotic Symptoms in Rape SurvivorsAllan DiasNo ratings yet
- Antidepressants and InsomniaDocument9 pagesAntidepressants and InsomniaAllan DiasNo ratings yet
- The Management of Insomnia: An UpdateDocument4 pagesThe Management of Insomnia: An UpdateAllan DiasNo ratings yet
- Mania Aguda Meta Analise - CiprianiDocument10 pagesMania Aguda Meta Analise - CiprianiAllan DiasNo ratings yet
- Primary InsomniaDocument11 pagesPrimary InsomniaAllan DiasNo ratings yet
- EpilepsiaDocument16 pagesEpilepsiaAllan DiasNo ratings yet
- Psychosis of Epilepsy: A Neurologist'S Perspective: Epilepsy & Behavior Available Online at OnDocument7 pagesPsychosis of Epilepsy: A Neurologist'S Perspective: Epilepsy & Behavior Available Online at OnAllan DiasNo ratings yet
- Insomnia and Psychiatric DisordersDocument4 pagesInsomnia and Psychiatric DisordersAllan DiasNo ratings yet
- InsomniaDocument6 pagesInsomniaAllan DiasNo ratings yet
- Psychiatric Disorders Associated With EpilepsyDocument18 pagesPsychiatric Disorders Associated With EpilepsyAllan DiasNo ratings yet
- An Update On The Effect of Clinical Mastitis On The Welfare of Dairy Cows and Potential TherapiesDocument11 pagesAn Update On The Effect of Clinical Mastitis On The Welfare of Dairy Cows and Potential TherapiesLorena PinedaNo ratings yet
- Compound Sodium Lactate in FDocument5 pagesCompound Sodium Lactate in FAnjanieNo ratings yet
- Rorschach Inkblot TestDocument80 pagesRorschach Inkblot TestSahrish Ali100% (5)
- Siddha Applied Science InstituteDocument4 pagesSiddha Applied Science InstituteLagin DranNo ratings yet
- P CPLDocument10 pagesP CPLJean FlorencondiaNo ratings yet
- Psychooncology PsychoneuroimmunologyDocument4 pagesPsychooncology PsychoneuroimmunologypazNo ratings yet
- Clinical Guidelines Diagnosis and Treatment ManualDocument324 pagesClinical Guidelines Diagnosis and Treatment Manual733No ratings yet
- SelfefficacyDocument4 pagesSelfefficacyapi-481958145No ratings yet
- Handbook of Inter DermDocument238 pagesHandbook of Inter Dermhesham100% (1)
- Common Sports InjuriesDocument24 pagesCommon Sports InjuriesChris PatlingraoNo ratings yet
- C Ompt BrocureDocument3 pagesC Ompt BrocureArya WigunaNo ratings yet
- Nursing Documentation ReportDocument4 pagesNursing Documentation ReportRicco Valentino CoenraadNo ratings yet
- The Man Who Mistook His Wife For A Hat and Other Clinical TalesDocument13 pagesThe Man Who Mistook His Wife For A Hat and Other Clinical TalesJustice Guinamant11% (53)
- Porter Macy General ResumeDocument2 pagesPorter Macy General Resumeapi-404457470No ratings yet
- 2015 Hrinj DrugsDocument303 pages2015 Hrinj Drugsprahul2588100% (1)
- Medical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 40Document9 pagesMedical-Surgical Nursing Assessment and Management of Clinical Problems 9e Chapter 40sarasjunkNo ratings yet
- David Macey Franz FannonDocument10 pagesDavid Macey Franz FannonVasiliki PetsaNo ratings yet
- DivyaDocument15 pagesDivyaSAMIKSHA SARAOGI 1823326No ratings yet
- Tickler PDFDocument177 pagesTickler PDFQueenie FarrahNo ratings yet
- Nursing Math Practice Questions, Answers, and TechniquesDocument118 pagesNursing Math Practice Questions, Answers, and Techniquesyaneidys perezNo ratings yet
- The Effects of The CORE Programme On Pain at Rest, Movement-Induced and Secondary Pain, Active Range of Motion, and Proprioception in Female Office Workers With Chronic Low Back Pa..Document11 pagesThe Effects of The CORE Programme On Pain at Rest, Movement-Induced and Secondary Pain, Active Range of Motion, and Proprioception in Female Office Workers With Chronic Low Back Pa..ilhamNo ratings yet
- Fibromyalgia: Points To Remember About FibromyalgiaDocument6 pagesFibromyalgia: Points To Remember About FibromyalgiaeliseeaNo ratings yet
- Management of Patients With Cerebrovascular Disorders: Ariel M. Ortuoste, RN, ManDocument115 pagesManagement of Patients With Cerebrovascular Disorders: Ariel M. Ortuoste, RN, ManarielleortuosteNo ratings yet
- Internet Mental Health Quality of Life ScaleDocument4 pagesInternet Mental Health Quality of Life Scaleapi-234715250No ratings yet
- Acupressure Points Archives - Page 3 of 9 - Modern ReflexologyDocument30 pagesAcupressure Points Archives - Page 3 of 9 - Modern ReflexologyMiodrag Kolakovic100% (1)
- An Introduction To AyurvedaDocument22 pagesAn Introduction To Ayurvedasnehalmaisuria100% (1)
- Contoh Soal TOEFL PT AskrindoDocument2 pagesContoh Soal TOEFL PT AskrindoDeni HarmokoNo ratings yet
- Health Education Substance AbuseDocument13 pagesHealth Education Substance Abusekiran mahal100% (2)
- Cafergot Patient eDocument3 pagesCafergot Patient eLaurentiu DinuNo ratings yet
- Nonvital Pulp Therapy On Primary TeethDocument15 pagesNonvital Pulp Therapy On Primary TeethJose RoldanNo ratings yet