You might also like
- HygieneDocument23 pagesHygienecaitlyntreacyNo ratings yet
- Hygiene PromotionDocument9 pagesHygiene PromotionAhmad Fahim ShahiNo ratings yet
- CommunityOrgnzng SlidesDocument85 pagesCommunityOrgnzng SlidesKhatlen BagaresNo ratings yet
- Nirmal Gram PuruskarDocument5 pagesNirmal Gram PuruskardreamzaliveNo ratings yet
- WASH WEBINAR Episode 2 - Hygiene Promotion in EmergenciesDocument52 pagesWASH WEBINAR Episode 2 - Hygiene Promotion in EmergenciesZakash AdowNo ratings yet
- Chapter 3Document108 pagesChapter 3Jerrie Mae MenciasNo ratings yet
- Hygiene - Introduction: ENVR 890 Mark D. Sobsey Spring, 2007Document28 pagesHygiene - Introduction: ENVR 890 Mark D. Sobsey Spring, 2007mahe_sce4702No ratings yet
- Wash 7Document22 pagesWash 7mrdaauud09No ratings yet
- Sphere Standards: Water Supply, Sanitation and Hygiene Promotion (WASH)Document29 pagesSphere Standards: Water Supply, Sanitation and Hygiene Promotion (WASH)Sote BrilloNo ratings yet
- Affordable Access To Adequate Wash FacilitiesDocument23 pagesAffordable Access To Adequate Wash FacilitiesJoseph GichehaNo ratings yet
- People Managed Environmental Sanitation BKD Raja April 2010Document15 pagesPeople Managed Environmental Sanitation BKD Raja April 2010Bkd RajaNo ratings yet
- International University Sek Environmental Sanitation Ii Group ADocument10 pagesInternational University Sek Environmental Sanitation Ii Group AVicky JimenezNo ratings yet
- Mediterranean Health Journal, 1999, 5:168-176Document6 pagesMediterranean Health Journal, 1999, 5:168-176Marz AcopNo ratings yet
- Mid Exam Environmental SanitationDocument3 pagesMid Exam Environmental SanitationAndresurya PradanaNo ratings yet
- Water Sanitation Hygiene Guidelines Global Grant Funding en PDFDocument53 pagesWater Sanitation Hygiene Guidelines Global Grant Funding en PDFcwchiascribd99No ratings yet
- Maldives SSHE GuidelinesDocument8 pagesMaldives SSHE GuidelinesAnup SahooNo ratings yet
- Proposed Study To Assess The Environmental Sanitation Needs of Ghanaian CommunitiesDocument20 pagesProposed Study To Assess The Environmental Sanitation Needs of Ghanaian CommunitiesRobertus Wisnu WijayaNo ratings yet
- CONSERVANCYDocument7 pagesCONSERVANCYrodgers omondiNo ratings yet
- Wash in Schools and CommunitiesDocument61 pagesWash in Schools and Communitiesदिपेश राईNo ratings yet
- Report For Practical Placement From 16th Jan To 3rd March 2017Document20 pagesReport For Practical Placement From 16th Jan To 3rd March 2017Patrick MugoNo ratings yet
- A Possible Framework For NG-CARES DLI 1.4 Nutrition Sector by Josephine Ayuk PH.DDocument33 pagesA Possible Framework For NG-CARES DLI 1.4 Nutrition Sector by Josephine Ayuk PH.DJosephine AyukNo ratings yet
- Central Java and Special Region of Yogyakarta: Environmental Services ProgramDocument2 pagesCentral Java and Special Region of Yogyakarta: Environmental Services ProgrammuhammadnainNo ratings yet
- 1.sanitation Policy and The MDGsDocument22 pages1.sanitation Policy and The MDGssofianina05No ratings yet
- Action Plan Based From Prioritized Problem IdentifiedDocument12 pagesAction Plan Based From Prioritized Problem IdentifiedCristina L. JaysonNo ratings yet
- Action Plan Shreya BhatDocument5 pagesAction Plan Shreya BhatShreeya BhatNo ratings yet
- Community Health RevisionDocument25 pagesCommunity Health RevisionfxbukenyaNo ratings yet
- WinsDocument31 pagesWinsKathleen Faith Blanco VergaraNo ratings yet
- MeasurementDocument1 pageMeasurementgabrielNo ratings yet
- Group 4Document59 pagesGroup 4Esmel Jane Cañedo PeñaflorNo ratings yet
- CLTsDocument16 pagesCLTsrodgers omondiNo ratings yet
- Cleanliness Throughout Life: The Importance of Showering from Childhood to AdulthoodFrom EverandCleanliness Throughout Life: The Importance of Showering from Childhood to AdulthoodNo ratings yet
- Sustainable Development Goals No. 1: Installation of Solar Panel On Rooftop For Electricity Generation Resouces RequiredDocument10 pagesSustainable Development Goals No. 1: Installation of Solar Panel On Rooftop For Electricity Generation Resouces Requiredrinkuamit71No ratings yet
- Risk Midterm Nov 6Document8 pagesRisk Midterm Nov 6Bern ConcepcionNo ratings yet
- WASH in Schools PDFDocument56 pagesWASH in Schools PDFakhilkuwar100% (2)
- Water Sanitation Group 3Document14 pagesWater Sanitation Group 3redhokojaNo ratings yet
- Health and Hygiene Promotion Best Practices and Lessons LearnedDocument56 pagesHealth and Hygiene Promotion Best Practices and Lessons LearnedSTBM IndonesiaNo ratings yet
- CHP4 - Low ResDocument24 pagesCHP4 - Low ResJunaid ZafarNo ratings yet
- NSTP 6Document3 pagesNSTP 6ANa AntonioNo ratings yet
- WORLD BANK 2007 Hygiene and Sanitation PromotionDocument24 pagesWORLD BANK 2007 Hygiene and Sanitation PromotionmesselecwNo ratings yet
- Activity 1 ObjectiveDocument6 pagesActivity 1 ObjectiveRei Allen RodriguezNo ratings yet
- Water, Sanitation and Hygiene Education in School: A Project Proposal ONDocument10 pagesWater, Sanitation and Hygiene Education in School: A Project Proposal ONsitheeqNo ratings yet
- Sustainable Rural Water, Sanitation and Hygiene Project PROPOSALDocument13 pagesSustainable Rural Water, Sanitation and Hygiene Project PROPOSALLawrence WatssonNo ratings yet
- Family Nursing Care Plan (Copy)Document3 pagesFamily Nursing Care Plan (Copy)Christine Anne RelayoNo ratings yet
- Project Title:: An Evaluation of The WorldDocument23 pagesProject Title:: An Evaluation of The WorldKofi AsamoahNo ratings yet
- Hygiene Promotion in EmergenciesDocument4 pagesHygiene Promotion in EmergenciesBlessing KanengoniNo ratings yet
- Cholera Hosp M'Document17 pagesCholera Hosp M'sandeshNo ratings yet
- Global Health Intervention Proposal Indonesias Total Sanitation Program 1Document5 pagesGlobal Health Intervention Proposal Indonesias Total Sanitation Program 1api-549315638No ratings yet
- Hygiene and Sanitation Are Essential To Good HealthDocument2 pagesHygiene and Sanitation Are Essential To Good HealthCharie Mae Gaurana BarbaNo ratings yet
- Community Water Supply and Sanitation (WSEE 3143) : Chapter OneDocument20 pagesCommunity Water Supply and Sanitation (WSEE 3143) : Chapter Onejebril yusufNo ratings yet
- Hvchap 9Document8 pagesHvchap 9Ma Michelle FranciscoNo ratings yet
- Health Promotion StratagiesDocument19 pagesHealth Promotion StratagiesDawud AsnakewNo ratings yet
- Indicators For Monitoring Hygiene PromotionDocument5 pagesIndicators For Monitoring Hygiene PromotionAbdullah SharifiNo ratings yet
- Training For Hygiene Promotion. Part 2: Useful To KnowDocument40 pagesTraining For Hygiene Promotion. Part 2: Useful To KnowOswar Mungkasa100% (3)
- Community Health NursingDocument40 pagesCommunity Health NursingSherlyn PedidaNo ratings yet
- Community Health Nursing Process0Document59 pagesCommunity Health Nursing Process0Mukul Thakur100% (1)
- Community Health Nursing Process: Dr. Maheswari JaikumarDocument59 pagesCommunity Health Nursing Process: Dr. Maheswari JaikumarSheryl Joy Soriano100% (1)
- L3 Health EducationDocument18 pagesL3 Health EducationBianca GeagoniaNo ratings yet
- Models of Disease Prevention Strategies 1st YearDocument64 pagesModels of Disease Prevention Strategies 1st YearM Zohaib Irshad AhmadNo ratings yet
- Mainstreaming Water Safety Plans in ADB Water Sector Projects: Lessons and ChallengesFrom EverandMainstreaming Water Safety Plans in ADB Water Sector Projects: Lessons and ChallengesNo ratings yet
- WALLPRES ExcavationDocument11 pagesWALLPRES ExcavationShekh Muhsen Uddin AhmedNo ratings yet
- Legend For Electrical Plan: General NotesDocument3 pagesLegend For Electrical Plan: General NotesShekh Muhsen Uddin AhmedNo ratings yet
- Channai MetroDocument11 pagesChannai MetroShekh Muhsen Uddin AhmedNo ratings yet
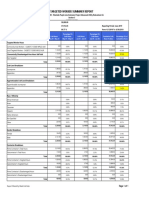
- Targeted Worker Summary Report: Economically Disadvantaged Area Hours SubtotalDocument1 pageTargeted Worker Summary Report: Economically Disadvantaged Area Hours SubtotalShekh Muhsen Uddin AhmedNo ratings yet
- A Time History Analysis Method-4689Document8 pagesA Time History Analysis Method-4689Shekh Muhsen Uddin AhmedNo ratings yet
- Column Layout PlanDocument1 pageColumn Layout PlanShekh Muhsen Uddin Ahmed0% (1)
- Pile DetailsDocument1 pagePile DetailsShekh Muhsen Uddin AhmedNo ratings yet
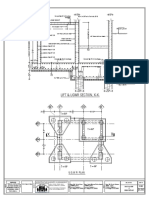
- Under Ground Reservoir DetailsDocument1 pageUnder Ground Reservoir DetailsShekh Muhsen Uddin AhmedNo ratings yet
- b2b SpliceDocument5 pagesb2b SpliceShekh Muhsen Uddin AhmedNo ratings yet
- b2b SpliceDocument42 pagesb2b SpliceShekh Muhsen Uddin AhmedNo ratings yet
- Materials Journal Keyword Index 2013 PDFDocument15 pagesMaterials Journal Keyword Index 2013 PDFShekh Muhsen Uddin AhmedNo ratings yet
- Ubc 97 Type 1 Irregularity CheckDocument11 pagesUbc 97 Type 1 Irregularity CheckShekh Muhsen Uddin AhmedNo ratings yet
- Torsional Irregularity Plan ASCE 7-10 EC8Document11 pagesTorsional Irregularity Plan ASCE 7-10 EC8Shekh Muhsen Uddin AhmedNo ratings yet
- ETABS Case StudyDocument45 pagesETABS Case StudyShekh Muhsen Uddin Ahmed100% (1)
- Pavement Design Methods 2 PDFDocument47 pagesPavement Design Methods 2 PDFShekh Muhsen Uddin AhmedNo ratings yet
- Assessment of Knowledge of Chronic Kidney Disease PDFDocument7 pagesAssessment of Knowledge of Chronic Kidney Disease PDFمالك مناصرةNo ratings yet
- Placebo-Controlled Trial of Amantadine For Severe Traumatic Brain Injury - NEJMDocument2 pagesPlacebo-Controlled Trial of Amantadine For Severe Traumatic Brain Injury - NEJMJamesHowsonNo ratings yet
- Stock Price Prediction Using Machine LearningDocument26 pagesStock Price Prediction Using Machine LearninganiNo ratings yet
- Geography Paper 4 Flashcards-2Document16 pagesGeography Paper 4 Flashcards-2faryal khanNo ratings yet
- Bellaachia PDFDocument4 pagesBellaachia PDFDr-Rabia AlmamalookNo ratings yet
- Analysis of Cesarean Section Rate - According To Robson's 10-Group ClassificationDocument4 pagesAnalysis of Cesarean Section Rate - According To Robson's 10-Group ClassificationMahavir GemavatNo ratings yet
- Steps in Literature Review WritingDocument6 pagesSteps in Literature Review Writingafmzzqrhardloa100% (1)
- Intentional IgnoranceDocument41 pagesIntentional IgnoranceCat SkullNo ratings yet
- A Conceptual Analysis of The Oceanic Fee PDFDocument30 pagesA Conceptual Analysis of The Oceanic Fee PDFgormatrNo ratings yet
- LP sensitivity-ORDocument13 pagesLP sensitivity-ORAdeel KhanNo ratings yet
- Module 1: Nature of Inquiry and Research What's MoreDocument6 pagesModule 1: Nature of Inquiry and Research What's MoreShaharmie Garcia100% (1)
- Rosemarie Rizzo Parse TheoryDocument3 pagesRosemarie Rizzo Parse TheoryKhrysta CaboNo ratings yet
- 3M AnalysisDocument5 pages3M AnalysisAritra BanerjeeNo ratings yet
- Advance Accounting Theory - Research ReportDocument10 pagesAdvance Accounting Theory - Research ReportAvinash VenkatNo ratings yet
- Vacuum Technology and Space Simulation NASA BookDocument315 pagesVacuum Technology and Space Simulation NASA BookDaylenO100% (1)
- The Environmental Audit Report (External Audit)Document3 pagesThe Environmental Audit Report (External Audit)Sheyyan TanNo ratings yet
- Program Hivr4p2018Document90 pagesProgram Hivr4p2018jadwongscribdNo ratings yet
- Newton's Principia - Red Light RobberDocument14 pagesNewton's Principia - Red Light RobberBruno RodriguezNo ratings yet
- Analysis of Consumer Behaviour OnlineDocument6 pagesAnalysis of Consumer Behaviour OnlineKelly NguyenNo ratings yet
- Guidance For Treatment of SSCs - ML12095A362Document134 pagesGuidance For Treatment of SSCs - ML12095A362Fernando DiezNo ratings yet
- Effect of A Musicians Exercise Intervention On Performance-Related Musculoskeletal DisordersDocument9 pagesEffect of A Musicians Exercise Intervention On Performance-Related Musculoskeletal DisordersBruni LopezNo ratings yet
- Malaysia Asian Barometer Survey Wave 5 2019Document43 pagesMalaysia Asian Barometer Survey Wave 5 2019emir.izatNo ratings yet
- Day Et Al 2008Document22 pagesDay Et Al 2008teddymcvNo ratings yet
- Plant Disease Detection Using Drones in Precision AgricultureDocument20 pagesPlant Disease Detection Using Drones in Precision AgricultureDavid Castorena MinorNo ratings yet
- Facility Layout Case StudyDocument8 pagesFacility Layout Case StudyHitesh SinglaNo ratings yet
- Fieldwork Packet 512 F 15Document12 pagesFieldwork Packet 512 F 15api-403294812No ratings yet
- Outsourcing Mini LessonDocument2 pagesOutsourcing Mini Lessonapi-270236691No ratings yet
- Swimlane DiagramsDocument11 pagesSwimlane DiagramsFelipe Rubio PlazaNo ratings yet
- 4.3 Components of A Research ProposalDocument7 pages4.3 Components of A Research ProposalROGEN MAE DIONIONo ratings yet
- FINAL-Nguyễn Quỳnh Chi-2013316663Document1 pageFINAL-Nguyễn Quỳnh Chi-2013316663Quỳnh Chi NguyễnNo ratings yet