You might also like
- Form2 - Application For Change of NameDocument2 pagesForm2 - Application For Change of Nameपरी रायNo ratings yet
- Applicant Personal Profile: Tourist Police Division Volunteer Application FormDocument3 pagesApplicant Personal Profile: Tourist Police Division Volunteer Application Formapi-27563929No ratings yet
- Self Declaration For Change of Name/ Gender Public NoticeDocument2 pagesSelf Declaration For Change of Name/ Gender Public Noticesanjay kumarNo ratings yet
- The West African Examinations Council Application Form: WAEC 85/3Document5 pagesThe West African Examinations Council Application Form: WAEC 85/3drlorenzNo ratings yet
- Hess Application Form PDFDocument4 pagesHess Application Form PDFMr Bona FideNo ratings yet
- New Joining Labouaar FormatDocument3 pagesNew Joining Labouaar FormatAshok SinghNo ratings yet
- Tenant Verification FormDocument1 pageTenant Verification FormRajiv Kumar Singh86% (22)
- Acte de DecesDocument2 pagesActe de DecesAnne Marie HoaroNo ratings yet
- Gurdians FormDocument1 pageGurdians FormofwetephaustineNo ratings yet
- Healthcare Realty Vacancy Application FormDocument4 pagesHealthcare Realty Vacancy Application FormMama TraoreNo ratings yet
- EAMS Member Application Form 2016Document1 pageEAMS Member Application Form 2016sinehardNo ratings yet
- Formats For Medico-Legal CertificationDocument84 pagesFormats For Medico-Legal CertificationJoshua D. ALARBANo ratings yet
- Radha PDFDocument1 pageRadha PDFGunjan DograNo ratings yet
- Report of Examination of A Female Victim of Sexual Assault: History Related To The Incident (As Stated by SubjectDocument3 pagesReport of Examination of A Female Victim of Sexual Assault: History Related To The Incident (As Stated by SubjectKashishNo ratings yet
- Guyana Police ForceDocument16 pagesGuyana Police Forcemorrislinden481No ratings yet
- Firearm Licence Application Form and Renewal of Licence - 2Document4 pagesFirearm Licence Application Form and Renewal of Licence - 2Jerome MassaweNo ratings yet
- Handout - Taking Patient's HistoryDocument1 pageHandout - Taking Patient's HistorySusheewa W. MulmuangNo ratings yet
- Guarantors FORM - Doc BADocument3 pagesGuarantors FORM - Doc BAagbaipissNo ratings yet
- LSC Global Logistics Application FormDocument3 pagesLSC Global Logistics Application FormDohan HarmandoNo ratings yet
- Case History and Examination Sheet For OralDocument3 pagesCase History and Examination Sheet For OralWegdan AldobaiNo ratings yet
- Emphasis Using InversionDocument5 pagesEmphasis Using InversionAndy QuickNo ratings yet
- Applicant Enquiry Form Dec 2018Document2 pagesApplicant Enquiry Form Dec 2018zemmyNo ratings yet
- Ekvp FormDocument4 pagesEkvp FormkahawapoNo ratings yet
- Application Format: Name of The Post Applied ForDocument2 pagesApplication Format: Name of The Post Applied ForArijit ShomeNo ratings yet
- Application Form VacancyDocument4 pagesApplication Form VacancySuchita HenrageNo ratings yet
- Protocol BluebookDocument16 pagesProtocol BluebookItz D LifeNo ratings yet
- Southsea Skatepark - Application FormDocument4 pagesSouthsea Skatepark - Application FormkadeNo ratings yet
- Rana Hospital: Patient Registration RecordDocument1 pageRana Hospital: Patient Registration RecordUmesh ChoudharyNo ratings yet
- Bail Bond - 14 PDFDocument2 pagesBail Bond - 14 PDFAnkit NandeNo ratings yet
- I. Transform The Sentences So That Their Meanings Stay The Same. Use Inversion With The Given WordDocument1 pageI. Transform The Sentences So That Their Meanings Stay The Same. Use Inversion With The Given WordSara Sofia TrochimiukNo ratings yet
- GP Referral Form 2023Document1 pageGP Referral Form 2023Rahul VishwanathNo ratings yet
- EOC Complaint FormDocument3 pagesEOC Complaint FormSameer AumNo ratings yet
- Agatha Legal: Solicitors & Advocates Law FirmDocument6 pagesAgatha Legal: Solicitors & Advocates Law FirmAGATHA LEGAL SOLICITORS & ADVOCATESNo ratings yet
- Photo: Form of Application For Admission To An Examination, December-2020Document1 pagePhoto: Form of Application For Admission To An Examination, December-2020Sur YadavNo ratings yet
- Prescribed Application Form ADocument3 pagesPrescribed Application Form ABhavish RamroopNo ratings yet
- Lesson 3 - Conditionals - WorksheetDocument9 pagesLesson 3 - Conditionals - Worksheetapi-550082451No ratings yet
- Application FormDocument3 pagesApplication FormsplashdownwaterparksNo ratings yet
- Emergency Contact FormDocument1 pageEmergency Contact FormMikeNo ratings yet
- Application FormDocument1 pageApplication FormSoumya Mariner DuttaNo ratings yet
- Rental Application: Primary ApplicantDocument3 pagesRental Application: Primary ApplicantJuan David Ramos LadinoNo ratings yet
- Complaints Record Form 17.1.01Document4 pagesComplaints Record Form 17.1.01Shahbaz AhmedNo ratings yet
- Carrying Out Examination) : (Please Type Four Copies From The Original Manuscript)Document1 pageCarrying Out Examination) : (Please Type Four Copies From The Original Manuscript)adangamo8No ratings yet
- Free Printable Legal Guardianship FormDocument2 pagesFree Printable Legal Guardianship Formlocke206No ratings yet
- Guardian-Form 1 PDFDocument2 pagesGuardian-Form 1 PDFSankar Nath Chakraborty0% (1)
- Application Form For Police VerificationDocument1 pageApplication Form For Police VerificationShabdobrahmaNo ratings yet
- Land Sale Agreement FormDocument1 pageLand Sale Agreement FormCOUNTY CYBER80% (51)
- Application Form: NAME OF DIPLOMADocument1 pageApplication Form: NAME OF DIPLOMASimbaNo ratings yet
- Ch. 31-39Document4 pagesCh. 31-39esraa haymanNo ratings yet
- Proforma For Defence Personnel: Under Calsue 6 (E) of Item 6 of Chapter of BrochureDocument3 pagesProforma For Defence Personnel: Under Calsue 6 (E) of Item 6 of Chapter of BrochureMohan JainNo ratings yet
- Uganda Visa FormDocument2 pagesUganda Visa FormKss selvaNo ratings yet
- Students Personal Details FormDocument2 pagesStudents Personal Details Formpuritymasika169No ratings yet
- Motor Acc CLM FormDocument3 pagesMotor Acc CLM FormSWISH IncNo ratings yet
- ApplicationDocument1 pageApplicationRachel Anne Harker- FergusonNo ratings yet
- New Loan Application FormDocument3 pagesNew Loan Application FormAKANKWASA ERASMUSNo ratings yet
- CCTV Consent FormDocument2 pagesCCTV Consent FormGam SaiiNo ratings yet
- Job Application Form-1Document4 pagesJob Application Form-1musa ballah koromaNo ratings yet
- FDIS Application FormDocument6 pagesFDIS Application FormaemNo ratings yet
- Centenary Bank Head Office Application For Employment Form: Confidential - ExternalDocument3 pagesCentenary Bank Head Office Application For Employment Form: Confidential - ExternalTom SesenteNo ratings yet
- Heard About What Happened From SomeoneDocument6 pagesHeard About What Happened From Someoneapi-2606993No ratings yet
- Separation of Powers in The Australian ConstitutioDocument19 pagesSeparation of Powers in The Australian ConstitutioTerry LollbackNo ratings yet
- Molloy MartialArtsMateriality 2008Document20 pagesMolloy MartialArtsMateriality 2008Terry LollbackNo ratings yet
- POSSIBLE GUIDANCE FROM Roman LawDocument14 pagesPOSSIBLE GUIDANCE FROM Roman LawTerry LollbackNo ratings yet
- Commonwealth Ombudsman 1988Document2 pagesCommonwealth Ombudsman 1988Terry LollbackNo ratings yet
- Recognition of Foreign DivorcesDocument19 pagesRecognition of Foreign DivorcesTerry LollbackNo ratings yet
- 1996mixed Results For Phone Fault Repair and Connection Customer SatisfactionDocument1 page1996mixed Results For Phone Fault Repair and Connection Customer SatisfactionTerry LollbackNo ratings yet
- New Community Radio Service For Oatlands1996Document1 pageNew Community Radio Service For Oatlands1996Terry LollbackNo ratings yet
- Filipinos in Nueva Espaã A: Filipino-Mexican Relations, Mestizaje, and Identity in Colonial and Contemporary MexicoDocument29 pagesFilipinos in Nueva Espaã A: Filipino-Mexican Relations, Mestizaje, and Identity in Colonial and Contemporary MexicoTerry LollbackNo ratings yet
- MOLLOY SwordsSwordsmanshipAegean 2010Document27 pagesMOLLOY SwordsSwordsmanshipAegean 2010Terry LollbackNo ratings yet
- Gen F QLD Stat DecDocument1 pageGen F QLD Stat DecTerry LollbackNo ratings yet
- Housing Market Update: Property Investor SummitDocument35 pagesHousing Market Update: Property Investor SummitTerry LollbackNo ratings yet
- Nla - News Article13325849.3 LollbackDocument1 pageNla - News Article13325849.3 LollbackTerry LollbackNo ratings yet
- Position Description Student Recruitment and Marketing Manager CHC OperationsDocument6 pagesPosition Description Student Recruitment and Marketing Manager CHC OperationsTerry LollbackNo ratings yet
- Quick Reference Guide For Agents: Be What Want To BeDocument16 pagesQuick Reference Guide For Agents: Be What Want To BeTerry LollbackNo ratings yet
- Pressure Point TrumaDocument4 pagesPressure Point TrumaTerry LollbackNo ratings yet
- Takagiryu HistoryDocument10 pagesTakagiryu HistoryTerry LollbackNo ratings yet
- Bang Bang He Shot Me Down Can The Pistol Be Studied As A Historic European Martial ArtDocument5 pagesBang Bang He Shot Me Down Can The Pistol Be Studied As A Historic European Martial ArtTerry LollbackNo ratings yet
- EOI BSC Donation FormDocument8 pagesEOI BSC Donation FormTerry LollbackNo ratings yet
- Eligible Course List Fact Sheet 0Document22 pagesEligible Course List Fact Sheet 0Terry LollbackNo ratings yet
- Depot - Wheelie Bin Request FormDocument1 pageDepot - Wheelie Bin Request FormTerry LollbackNo ratings yet
- Grafton 131220 Community Liason PlanDocument15 pagesGrafton 131220 Community Liason PlanTerry LollbackNo ratings yet
- Grafton Ma Hoo Suc MapDocument1 pageGrafton Ma Hoo Suc MapTerry LollbackNo ratings yet
- Business Assistance Brochure A Guide To Council ServicesDocument9 pagesBusiness Assistance Brochure A Guide To Council ServicesTerry LollbackNo ratings yet
- Application For Use of Council Controlled Parks and ReservesDocument5 pagesApplication For Use of Council Controlled Parks and ReservesTerry LollbackNo ratings yet
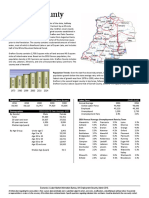
- Grafton County Grafton County Grafton County Grafton County: Population (US Census Bureau) Labor Force (Nhes-Elmi)Document5 pagesGrafton County Grafton County Grafton County Grafton County: Population (US Census Bureau) Labor Force (Nhes-Elmi)Terry LollbackNo ratings yet
- Failure To Provide Bank Account Details May Result in A Delay in Your RefundDocument2 pagesFailure To Provide Bank Account Details May Result in A Delay in Your RefundTerry Lollback100% (2)