You might also like
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Entrance Exam Candidate's Name Father's Name Mother's Name Date of Birth Mobile Number AddressDocument4 pagesEntrance Exam Candidate's Name Father's Name Mother's Name Date of Birth Mobile Number AddressMeckange PotharajuNo ratings yet
- Testing SyllabusDocument4 pagesTesting Syllabussudhakar kakunuriNo ratings yet
- EasyBuilderPro UserManual enDocument864 pagesEasyBuilderPro UserManual enshashirajNo ratings yet
- Crest CRT Cpsa Technical Syllabus 2.0Document20 pagesCrest CRT Cpsa Technical Syllabus 2.0Azaz Ahmed DobiwalaNo ratings yet
- MilestoneXProtectSmartClient Users Manual en-US PDFDocument150 pagesMilestoneXProtectSmartClient Users Manual en-US PDFMarian PatracutaNo ratings yet
- 4 Pax 1Document2 pages4 Pax 1Ahsan AliNo ratings yet
- Interior Lighting System: SectionDocument81 pagesInterior Lighting System: SectionMax RughfiddNo ratings yet
- Toshiba e-STUDIO Safety Information GuideDocument26 pagesToshiba e-STUDIO Safety Information GuideMikeNo ratings yet
- Manual TCG220Document61 pagesManual TCG220David LezcanoNo ratings yet
- KT Biometric SOP V1.0Document3 pagesKT Biometric SOP V1.0FCI chhola Office bhopalNo ratings yet
- Khyati Product Project ReportDocument67 pagesKhyati Product Project ReportAkshay Bhatt100% (3)
- The CISO ViewDocument18 pagesThe CISO ViewPradeep JoshiNo ratings yet
- SLSP Esubmission Confirmation - 2018Document2 pagesSLSP Esubmission Confirmation - 2018Dennis CreerNo ratings yet
- PH PC-Stations 76Document478 pagesPH PC-Stations 76Tiago Oliveira100% (1)
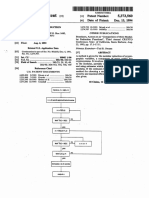
- Us 5373560Document20 pagesUs 5373560cbetterNo ratings yet
- Week 7 Chapter 7: Guest RegistrationDocument12 pagesWeek 7 Chapter 7: Guest RegistrationechxNo ratings yet
- Info Security Quiz 1Document3 pagesInfo Security Quiz 1asmal.saarahNo ratings yet
- Introduction To CybersecurityDocument46 pagesIntroduction To CybersecurityDevansh JainNo ratings yet
- Undertaking 2024 2025Document1 pageUndertaking 2024 2025Leoni FrancNo ratings yet
- Dutch Consulate Passport CommunicationsDocument3 pagesDutch Consulate Passport CommunicationsLisette MuntslagNo ratings yet
- Booklet (Anti-Tinnitus Sound System) v15 PDFDocument35 pagesBooklet (Anti-Tinnitus Sound System) v15 PDFAndrei OanceaNo ratings yet
- Canada Visitor Visa Procedure and ChecklistDocument12 pagesCanada Visitor Visa Procedure and ChecklistmrinalNo ratings yet
- Other Data Mancon ReportDocument8 pagesOther Data Mancon ReportlezzzzhhhhaaabaybNo ratings yet
- Synology Drive WPDocument18 pagesSynology Drive WPMark Brown100% (1)
- CertificationofAddressHSMV71120 PDFDocument1 pageCertificationofAddressHSMV71120 PDFHerb DettmerNo ratings yet
- Security and Cryptography: OrganizationDocument27 pagesSecurity and Cryptography: OrganizationkitoNo ratings yet
- Design of Arduino Based Home Automation Systems Incorporating Identity DetectionDocument77 pagesDesign of Arduino Based Home Automation Systems Incorporating Identity DetectionShania MagsinoNo ratings yet
- Software Requirement Specification For Online Shopping SystemDocument8 pagesSoftware Requirement Specification For Online Shopping Systempawansingh100% (1)
- Slinger Signaller BanksmanDocument88 pagesSlinger Signaller BanksmanAhmed GaballaNo ratings yet
- Web Check-In Help: Tutorial 2. Web Check-In Help: Frequently Asked Questions (FAQ)Document34 pagesWeb Check-In Help: Tutorial 2. Web Check-In Help: Frequently Asked Questions (FAQ)one kilometerNo ratings yet