You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- What Is Intelligence?Document4 pagesWhat Is Intelligence?Michellene TadleNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Heres The Rest of Him-Kent H Steffgen-1968-192pgs-GOVDocument192 pagesHeres The Rest of Him-Kent H Steffgen-1968-192pgs-GOVJeffrey Smith100% (1)
- Education Is Better Than MoneyDocument6 pagesEducation Is Better Than MoneyMichellene Tadle71% (14)
- Environmental Science (Module 3)Document22 pagesEnvironmental Science (Module 3)Michellene Tadle100% (1)
- Environmental Science (Module 1)Document35 pagesEnvironmental Science (Module 1)Michellene Tadle67% (21)
- TRAFFIC JUNCTION SIMULATION-projectDocument45 pagesTRAFFIC JUNCTION SIMULATION-projectmacklyn tyan100% (2)
- Rizal in EuropeDocument10 pagesRizal in EuropeMichellene TadleNo ratings yet
- Reincarnated As A Sword Volume 12Document263 pagesReincarnated As A Sword Volume 12Phil100% (1)
- IndulgenceDocument4 pagesIndulgenceMichellene TadleNo ratings yet
- Environmental Science (Module 2)Document19 pagesEnvironmental Science (Module 2)Michellene Tadle100% (2)
- Rizal's BoyhoodDocument11 pagesRizal's BoyhoodMichellene Tadle0% (1)
- Read Aloud: Reading ComprehensionDocument3 pagesRead Aloud: Reading ComprehensionMichellene TadleNo ratings yet
- Chemistry LabDocument1 pageChemistry LabMichellene TadleNo ratings yet
- Reading Comprehension Skills For English Language LearnersDocument5 pagesReading Comprehension Skills For English Language LearnersMichellene TadleNo ratings yet
- Descriptive Definition of Original SinDocument13 pagesDescriptive Definition of Original SinMichellene TadleNo ratings yet
- First Aid QuizDocument2 pagesFirst Aid QuizMichellene Tadle100% (1)
- Logical Validity Can at Least Roughly Be Defined As The Property An Argument (A Set of Sentences Among WhichDocument1 pageLogical Validity Can at Least Roughly Be Defined As The Property An Argument (A Set of Sentences Among WhichMichellene TadleNo ratings yet
- Memories of My TownDocument8 pagesMemories of My TownMichellene TadleNo ratings yet
- 8 CHN SkillsDocument15 pages8 CHN SkillsMichellene TadleNo ratings yet
- 11 General OrdersDocument1 page11 General OrdersMichellene TadleNo ratings yet
- Mental Status ExamDocument14 pagesMental Status ExamMichellene TadleNo ratings yet
- Food Hydrocolloids: Eric DickinsonDocument13 pagesFood Hydrocolloids: Eric DickinsonAndres Felipe Rojas RodriguezNo ratings yet
- Ptfe ManufacturingDocument16 pagesPtfe ManufacturingKokki Kumar Dpce100% (1)
- Peter John G. Dadula: (Career Objective) (Educati ON)Document1 pagePeter John G. Dadula: (Career Objective) (Educati ON)Jericho JacalneNo ratings yet
- Marketing Ethics Amal 12-09-10Document11 pagesMarketing Ethics Amal 12-09-10amalroy1986No ratings yet
- Mba Final Project DaviDocument61 pagesMba Final Project DaviHarjagjeet singh0% (1)
- General Service ListDocument77 pagesGeneral Service ListMustafa GüneşNo ratings yet
- Dina Iordanova - Women in Balkan Cinema, Surviving On The MarginsDocument17 pagesDina Iordanova - Women in Balkan Cinema, Surviving On The MarginsimparatulverdeNo ratings yet
- Product Manual 85018V2 (Revision F) : 505E Digital Governor For Extraction Steam TurbinesDocument160 pagesProduct Manual 85018V2 (Revision F) : 505E Digital Governor For Extraction Steam Turbinesrahilshah100No ratings yet
- Self Regulatory Games For ChildrenDocument5 pagesSelf Regulatory Games For ChildrenKIP-HIDRAULIKA MNo ratings yet
- BÀI TẬP ÔN HSG TỈNHDocument12 pagesBÀI TẬP ÔN HSG TỈNHnguyễn Đình TuấnNo ratings yet
- How The Tortoise Got Its ScarsDocument3 pagesHow The Tortoise Got Its ScarsAngelenwNo ratings yet
- Quality Reliability Eng - 2021 - Saha - Parametric Inference of The Loss Based Index CPM For Normal DistributionDocument27 pagesQuality Reliability Eng - 2021 - Saha - Parametric Inference of The Loss Based Index CPM For Normal DistributionShweta SinghNo ratings yet
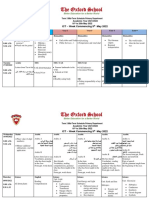
- Term 3 Mid-Term Assessment ScheduleDocument9 pagesTerm 3 Mid-Term Assessment ScheduleRabia MoeedNo ratings yet
- Job AnalysisDocument17 pagesJob AnalysisMd. Mezba Uddin ShaonNo ratings yet
- 08 03 Runge-Kutta 2nd Order MethodDocument11 pages08 03 Runge-Kutta 2nd Order MethodJohn Bofarull GuixNo ratings yet
- Voloxal TabletsDocument9 pagesVoloxal Tabletselcapitano vegetaNo ratings yet
- Group No. - Leader: MembersDocument7 pagesGroup No. - Leader: MembersJONATHAN NACHORNo ratings yet
- Competition Commission of India: Mahendra SoniDocument16 pagesCompetition Commission of India: Mahendra SoniSuman sharmaNo ratings yet
- Annual Report 2017 05 PDFDocument85 pagesAnnual Report 2017 05 PDFdewiNo ratings yet
- Child and Adolescent Psychiatry ST1Document6 pagesChild and Adolescent Psychiatry ST1danielNo ratings yet
- Film Viewing RomeroDocument3 pagesFilm Viewing RomeroJenesis MuescoNo ratings yet
- Mission: Children'SDocument36 pagesMission: Children'SWillian A. Palacio MurilloNo ratings yet
- Daily Lesson Log in Math 9Document13 pagesDaily Lesson Log in Math 9Marjohn PalmesNo ratings yet
- ST Learning Task 10Document6 pagesST Learning Task 10Jermaine DoloritoNo ratings yet
- Practice in KeyboardingDocument16 pagesPractice in KeyboardingRaymart GonzagaNo ratings yet
- Test 04 AnswerDocument16 pagesTest 04 AnswerCửu KhoaNo ratings yet
- Agostinis Et Al-2011-CA - A Cancer Journal For CliniciansDocument32 pagesAgostinis Et Al-2011-CA - A Cancer Journal For CliniciansKauniIsaacNo ratings yet