You might also like
- Brain Tumors in ChildrenFrom EverandBrain Tumors in ChildrenAmar GajjarNo ratings yet
- Multiple Myeloma and Other Plasma Cell NeoplasmsFrom EverandMultiple Myeloma and Other Plasma Cell NeoplasmsMeletios A. DimopoulosNo ratings yet
- MoyamoyaDocument11 pagesMoyamoyaSubashssNo ratings yet
- Causes Clinical and Imaging Characteristics of Moyamoya Disease in ChildrenDocument6 pagesCauses Clinical and Imaging Characteristics of Moyamoya Disease in ChildrenRiya CassendraNo ratings yet
- Children - Acute Transvers MyelitisDocument6 pagesChildren - Acute Transvers MyelitisHAKIMOPNo ratings yet
- Brain TumorsDocument12 pagesBrain Tumors36Kushal saNdHuNo ratings yet
- Achondroplasia Natural History Study (CLARITY)Document7 pagesAchondroplasia Natural History Study (CLARITY)jakelinelagoadvNo ratings yet
- Jurnal 1Document9 pagesJurnal 1AnnisNo ratings yet
- Cancers: New Developments in The Pathogenesis, Therapeutic Targeting, and Treatment of Pediatric MedulloblastomaDocument15 pagesCancers: New Developments in The Pathogenesis, Therapeutic Targeting, and Treatment of Pediatric MedulloblastomaSebastian SalvadorNo ratings yet
- Tumores CerebralesDocument24 pagesTumores CerebralesRocio LedesmaNo ratings yet
- Hemorrhagic Glioblastoma Multiform: Prevalence, Predisposing Factors and Prognosis Among Adult KFMC PatientsDocument15 pagesHemorrhagic Glioblastoma Multiform: Prevalence, Predisposing Factors and Prognosis Among Adult KFMC PatientsijasrjournalNo ratings yet
- Hemorrhagic Glioblastoma Multiform: Prevalence, Predisposing Factors and Prognosis Among Adult KFMC PatientsDocument15 pagesHemorrhagic Glioblastoma Multiform: Prevalence, Predisposing Factors and Prognosis Among Adult KFMC PatientsijasrjournalNo ratings yet
- ZH 804212003187Document19 pagesZH 804212003187Bismillah BerkahNo ratings yet
- Brain Tumor Thesis StatementDocument8 pagesBrain Tumor Thesis Statementchristinamartinspringfield100% (2)
- Medulloblastoma: Clinical and Biologic Aspects: Neuro-OncologyDocument19 pagesMedulloblastoma: Clinical and Biologic Aspects: Neuro-OncologyHilda Muhammad YusufNo ratings yet
- Eiichi Ishii (Eds.) - Hematological Disorders in Children - Pathogenesis and Treatment-Springer Singapore (2017)Document268 pagesEiichi Ishii (Eds.) - Hematological Disorders in Children - Pathogenesis and Treatment-Springer Singapore (2017)ZoraRosaNo ratings yet
- Juvenile Dermatomyositis and Polymyositis: Epidemiology, Pathogenesis, and Clinical ManifestationsDocument14 pagesJuvenile Dermatomyositis and Polymyositis: Epidemiology, Pathogenesis, and Clinical ManifestationsSanjuy GarzaNo ratings yet
- Pediatric Acute Transverse Myelitis Overview and Differential DiagnosisDocument12 pagesPediatric Acute Transverse Myelitis Overview and Differential Diagnosismmoraes0709No ratings yet
- Neuroblastoma Origin and Therapeutic Targets For IDocument26 pagesNeuroblastoma Origin and Therapeutic Targets For IRokia GhariebNo ratings yet
- Fimmu 13 915081Document15 pagesFimmu 13 915081Zakia MaharaniNo ratings yet
- Diagnostics 12 02064Document25 pagesDiagnostics 12 02064dptofisicaflorestaNo ratings yet
- Therapeutic Approach To The Management of Pediatric Demyelinating Disease: Multiple Sclerosis and Acute Disseminated EncephalomyelitisDocument12 pagesTherapeutic Approach To The Management of Pediatric Demyelinating Disease: Multiple Sclerosis and Acute Disseminated EncephalomyelitiscarlaNo ratings yet
- Otogenic Brain Abscess Our ExperienceDocument5 pagesOtogenic Brain Abscess Our ExperienceNeysaAzaliaEfrimaisaNo ratings yet
- Brainstem Gliomas: BackgroundDocument10 pagesBrainstem Gliomas: Backgroundanak99No ratings yet
- Global Differences in Risk Factors, Etiology, and Outcome of Ischemic Stroke in Young Adults-A Worldwide Meta-Analysis - The GOAL InitiativeDocument16 pagesGlobal Differences in Risk Factors, Etiology, and Outcome of Ischemic Stroke in Young Adults-A Worldwide Meta-Analysis - The GOAL InitiativeCARLOS BONILLANo ratings yet
- NIH Public Access: Author ManuscriptDocument22 pagesNIH Public Access: Author ManuscriptHumberto QuimeNo ratings yet
- Review Article: Recent Advances in Childhood Brain TumoursDocument10 pagesReview Article: Recent Advances in Childhood Brain Tumoursjosue_wigNo ratings yet
- Life 14 00367Document11 pagesLife 14 00367Shahmeer HassanNo ratings yet
- Rheumatic Heart Disease Anno 2020. Impacts of Gender and Migration On Epidemiology and Management (2020)Document9 pagesRheumatic Heart Disease Anno 2020. Impacts of Gender and Migration On Epidemiology and Management (2020)7 MNTNo ratings yet
- APJCP - Volume 20 - Issue 10 - Pages 2883-2890.pdf ELISA Glioma CitokinesDocument8 pagesAPJCP - Volume 20 - Issue 10 - Pages 2883-2890.pdf ELISA Glioma Citokinesplanhigion06No ratings yet
- Coppetal 2015 Nat Revs Disease Primers 20157Document67 pagesCoppetal 2015 Nat Revs Disease Primers 20157Nexi anessaNo ratings yet
- Isaacs2002Document13 pagesIsaacs2002FarhanNo ratings yet
- Epidemiology, Aetiology, and Management of IschaemicDocument12 pagesEpidemiology, Aetiology, and Management of IschaemicKhairunNisaNo ratings yet
- Review Article: Today and Future of Age-Related Macular DegenerationDocument9 pagesReview Article: Today and Future of Age-Related Macular DegenerationAngkat Prasetya Abdi NegaraNo ratings yet
- Acute Coagulopathy in Pediatric Trauma: ReviewDocument7 pagesAcute Coagulopathy in Pediatric Trauma: ReviewCarolina SartiniNo ratings yet
- MMD EpidDocument10 pagesMMD EpidGilbert Sterling OctaviusNo ratings yet
- Moyamoya Epidemiology, Presentation, and DiagnosisDocument9 pagesMoyamoya Epidemiology, Presentation, and DiagnosisshiloinNo ratings yet
- A Decade of Management of Subdural Haematoma in Children Aged 2 To 24 Months Hospitalized at The Paediatric Neurosurgery Department of La Timone Children's HospitalDocument8 pagesA Decade of Management of Subdural Haematoma in Children Aged 2 To 24 Months Hospitalized at The Paediatric Neurosurgery Department of La Timone Children's HospitalEditor IJTSRDNo ratings yet
- PHD Thesis LeukemiaDocument6 pagesPHD Thesis Leukemiaafjryccau100% (2)
- brb3 1291Document9 pagesbrb3 1291meyvitasNo ratings yet
- Introduction To Dendritic Cell Vaccines Immunotherapy For Glioblastoma Multiforme: A Novel ApproachDocument5 pagesIntroduction To Dendritic Cell Vaccines Immunotherapy For Glioblastoma Multiforme: A Novel ApproachparcoxssNo ratings yet
- prm/2018/11 4/prm 11 4 prm170481/prm 11 prm170481Document9 pagesprm/2018/11 4/prm 11 4 prm170481/prm 11 prm170481Putri Rizky AmaliaNo ratings yet
- Different Clinical Presentation and Management of Temporal Bone Fibrous Dysplasia in ChildrenDocument14 pagesDifferent Clinical Presentation and Management of Temporal Bone Fibrous Dysplasia in Childrensolikin ikinNo ratings yet
- An Overview of Meningiomas: ReviewDocument18 pagesAn Overview of Meningiomas: ReviewMuhammad Naqvi Al FarisiNo ratings yet
- Understanding and Treating Moyamoya Disease in ChildrenDocument11 pagesUnderstanding and Treating Moyamoya Disease in ChildrenFitriyana WinarnoNo ratings yet
- Review Article: Pediatric Multiple Sclerosis: Current Concepts and Consensus DefinitionsDocument24 pagesReview Article: Pediatric Multiple Sclerosis: Current Concepts and Consensus DefinitionsKelly GómezNo ratings yet
- Epidemiology, Pathogenesis, and Pathology of NeuroblastomaDocument21 pagesEpidemiology, Pathogenesis, and Pathology of NeuroblastomaHandre PutraNo ratings yet
- J BCMD 2017 03 003Document46 pagesJ BCMD 2017 03 003aliakbar178No ratings yet
- Safe and Sustainable: The Extracranial Approach Toward Frontoethmoidal Meningoencephalocele RepairDocument7 pagesSafe and Sustainable: The Extracranial Approach Toward Frontoethmoidal Meningoencephalocele RepairYovanka Naryai ManuhutuNo ratings yet
- NIH Public Access: NeuroblastomaDocument15 pagesNIH Public Access: NeuroblastomaMikael AngelooNo ratings yet
- Research Paper On Mitochondrial DiseaseDocument6 pagesResearch Paper On Mitochondrial Diseasegz91rnat100% (1)
- Clinical-Diagnostic Features of Duchenne Muscular Dystrophy in ChildrenDocument3 pagesClinical-Diagnostic Features of Duchenne Muscular Dystrophy in ChildrenFajri MuhammadNo ratings yet
- Risk Factors Association With Severity of White Matter Lesions On Magneticresonance Imaging 2327 5146 1000290Document7 pagesRisk Factors Association With Severity of White Matter Lesions On Magneticresonance Imaging 2327 5146 1000290Ranganathan Rma IyerNo ratings yet
- Xujiayuan Paper 3 BrainDocument15 pagesXujiayuan Paper 3 BrainxujiayuanNo ratings yet
- 2022 Janas NazeDocument10 pages2022 Janas NazeazizhamoudNo ratings yet
- 1.masas en CuelloDocument3 pages1.masas en CuelloIsaac TellezNo ratings yet
- Guideline On Acquired Temporomandibular Disorders in Infants, Children, and AdolescentsDocument7 pagesGuideline On Acquired Temporomandibular Disorders in Infants, Children, and AdolescentsSuaeni Kurnia WirdaNo ratings yet
- Perioperative Management of The Pediatric Patient With Traumatic Brain InjuryDocument14 pagesPerioperative Management of The Pediatric Patient With Traumatic Brain InjuryBaha MirzaeifarNo ratings yet
- Out PDFDocument11 pagesOut PDFyadiNo ratings yet
- The Pathogenesis of Port Wine Stain and Sturge Weber Syndrome: Complex Interactions Between Genetic Alterations and Aberrant MAPK and PI3K ActivationDocument17 pagesThe Pathogenesis of Port Wine Stain and Sturge Weber Syndrome: Complex Interactions Between Genetic Alterations and Aberrant MAPK and PI3K ActivationdzhzrnNo ratings yet
- Span of Control. Instructions Feed Downwards From One Level of ManagementDocument2 pagesSpan of Control. Instructions Feed Downwards From One Level of ManagementClaudia JessicaNo ratings yet
- Span of Control. Instructions Feed Downwards From One Level of ManagementDocument2 pagesSpan of Control. Instructions Feed Downwards From One Level of ManagementClaudia JessicaNo ratings yet
- Span of Control. Instructions Feed Downwards From One Level of ManagementDocument2 pagesSpan of Control. Instructions Feed Downwards From One Level of ManagementClaudia JessicaNo ratings yet
- Tokso OkularDocument13 pagesTokso OkularClaudia JessicaNo ratings yet
- Anatomy IlealDocument4 pagesAnatomy IlealClaudia JessicaNo ratings yet
- Anatomy IlealDocument4 pagesAnatomy IlealClaudia JessicaNo ratings yet
- Curling Ulcer 2Document6 pagesCurling Ulcer 2Claudia Jessica100% (1)
- AdvertisementsDocument1 pageAdvertisementsClaudia JessicaNo ratings yet
- Journal 5Document6 pagesJournal 5Claudia JessicaNo ratings yet
- AdvertisementsDocument1 pageAdvertisementsClaudia JessicaNo ratings yet
- AdvertisementsDocument1 pageAdvertisementsClaudia JessicaNo ratings yet
- AdvertisementsDocument1 pageAdvertisementsClaudia JessicaNo ratings yet
- Anatomy IlealDocument4 pagesAnatomy IlealClaudia JessicaNo ratings yet
- Journal 7Document8 pagesJournal 7Claudia JessicaNo ratings yet
- Journal 8Document7 pagesJournal 8Claudia JessicaNo ratings yet
- Journal 6Document7 pagesJournal 6Claudia JessicaNo ratings yet
- Journal 4Document5 pagesJournal 4Claudia JessicaNo ratings yet
- Journal 2Document8 pagesJournal 2Claudia JessicaNo ratings yet
- Anemia Pada Atrial Fibrilasi PDFDocument7 pagesAnemia Pada Atrial Fibrilasi PDFYunan Syahban MaskatNo ratings yet
- Increased Expressions of Integrin Subunit β1, β2 and β3 in Patients with Acute InfectionDocument5 pagesIncreased Expressions of Integrin Subunit β1, β2 and β3 in Patients with Acute InfectionClaudia JessicaNo ratings yet
- Managing Errors and ExceptionDocument12 pagesManaging Errors and ExceptionShanmuka Sreenivas100% (1)
- Ferobide Applications Brochure English v1 22Document8 pagesFerobide Applications Brochure English v1 22Thiago FurtadoNo ratings yet
- S-Sapfico-Satyanarayanamaterial 121212Document183 pagesS-Sapfico-Satyanarayanamaterial 121212mpsing1133No ratings yet
- Thermodynamics WorksheetDocument5 pagesThermodynamics WorksheetMalcolmJustMalcolmNo ratings yet
- Data Science ProjectsDocument3 pagesData Science ProjectsHanane GríssetteNo ratings yet
- Post Renaissance Architecture in EuropeDocument10 pagesPost Renaissance Architecture in Europekali_007No ratings yet
- PCM Cables: What Is PCM Cable? Why PCM Cables? Application?Document14 pagesPCM Cables: What Is PCM Cable? Why PCM Cables? Application?sidd_mgrNo ratings yet
- Rdramirez Aota 2018 Poster For PortfolioDocument1 pageRdramirez Aota 2018 Poster For Portfolioapi-437843157No ratings yet
- ABHA Coil ProportionsDocument5 pagesABHA Coil ProportionsOctav OctavianNo ratings yet
- Stratum CorneumDocument4 pagesStratum CorneumMuh Firdaus Ar-RappanyNo ratings yet
- Abas Drug Study Nicu PDFDocument4 pagesAbas Drug Study Nicu PDFAlexander Miguel M. AbasNo ratings yet
- Tata NanoDocument25 pagesTata Nanop01p100% (1)
- SPFL Monitoring ToolDocument3 pagesSPFL Monitoring ToolAnalyn EnriquezNo ratings yet
- BV DoshiDocument6 pagesBV DoshiNimNo ratings yet
- DBM Uv W ChartDocument2 pagesDBM Uv W ChartEddie FastNo ratings yet
- Springs: All India Distributer of NienhuisDocument35 pagesSprings: All India Distributer of NienhuisIrina DroliaNo ratings yet
- GrenTech Express Communication System Introduction 1.0Document30 pagesGrenTech Express Communication System Introduction 1.0Son NguyenNo ratings yet
- Economics Exam Technique GuideDocument21 pagesEconomics Exam Technique Guidemalcewan100% (5)
- OsciloscopioDocument103 pagesOsciloscopioFredy Alberto Gómez AlcázarNo ratings yet
- HR Practices in Public Sector Organisations: (A Study On APDDCF LTD.)Document28 pagesHR Practices in Public Sector Organisations: (A Study On APDDCF LTD.)praffulNo ratings yet
- Kortz Center GTA Wiki FandomDocument1 pageKortz Center GTA Wiki FandomsamNo ratings yet
- Previews 1633186 PreDocument11 pagesPreviews 1633186 PreDavid MorenoNo ratings yet
- SL Generator Ultrasunete RincoDocument2 pagesSL Generator Ultrasunete RincoDariaNo ratings yet
- Our Story Needs No Filter by Nagarkar SudeepDocument153 pagesOur Story Needs No Filter by Nagarkar SudeepKavya SunderNo ratings yet
- Employee of The Month.Document2 pagesEmployee of The Month.munyekiNo ratings yet
- A Project On "Automatic Water Sprinkler Based On Wet and Dry Conditions"Document28 pagesA Project On "Automatic Water Sprinkler Based On Wet and Dry Conditions"Srínívas SrínuNo ratings yet
- Less Homework More TroubleDocument7 pagesLess Homework More Troubleg697a0mw100% (1)
- Bharti Airtel Strategy FinalDocument39 pagesBharti Airtel Strategy FinalniksforloveuNo ratings yet
- Index: © Christopher Pitt 2018 C. Pitt, The Definitive Guide To AdonisjsDocument5 pagesIndex: © Christopher Pitt 2018 C. Pitt, The Definitive Guide To AdonisjsZidi BoyNo ratings yet
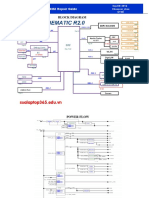
- Asus x453Document5 pagesAsus x453Rhiry Ntuh AthryNo ratings yet