You might also like
- Children's Perceptions of Parental Behavior MeasuredDocument13 pagesChildren's Perceptions of Parental Behavior MeasuredAlexandra Villarreal100% (1)
- Fiziologie Aplicata - 2019Document16 pagesFiziologie Aplicata - 2019RaduNo ratings yet
- 666 CDR - Scale PDFDocument10 pages666 CDR - Scale PDFIkanpaus Di BlogspotNo ratings yet
- 1 2018Document48 pages1 2018Lizz22No ratings yet
- Chou, H. L. The Moderating Effects of Parenting Styles On The Relation Between The Internet Attitudes and Internet Behaviors of Highschool Students in TaiwanArticle 2016Document11 pagesChou, H. L. The Moderating Effects of Parenting Styles On The Relation Between The Internet Attitudes and Internet Behaviors of Highschool Students in TaiwanArticle 2016novy loudoeNo ratings yet
- Eysenck Personality Questionnaire Revised (EPQ-R) - Measure Psychoticism, Neuroticism & ExtraversionDocument7 pagesEysenck Personality Questionnaire Revised (EPQ-R) - Measure Psychoticism, Neuroticism & ExtraversionNeha FloryNo ratings yet
- Gaf Guidelines To Determine Level of CareDocument2 pagesGaf Guidelines To Determine Level of Careapi-260339450No ratings yet
- Psychiatric Assessment Scale InfoDocument2 pagesPsychiatric Assessment Scale InfoRoxana SanduNo ratings yet
- Differences Between All Versions of DSMDocument6 pagesDifferences Between All Versions of DSMMahnoor BangushNo ratings yet
- Comparație Între SCID 5 RV Și SCID 5 CVDocument3 pagesComparație Între SCID 5 RV Și SCID 5 CVAdrianBelean100% (1)
- Epq-R (Forma Scurta)Document9 pagesEpq-R (Forma Scurta)minodoraNo ratings yet
- Dependenta de Jocuri de NorocDocument4 pagesDependenta de Jocuri de NorocAllen Wheeler100% (1)
- Hans J Eysenck and Raymond B Cattell On Inte 2016 Personality and IndividuDocument8 pagesHans J Eysenck and Raymond B Cattell On Inte 2016 Personality and IndividuPaula CelsieNo ratings yet
- T DR,,LT - N I - (. ,: B A, Arr&: - ,LQT Aor A # MFP# ADocument10 pagesT DR,,LT - N I - (. ,: B A, Arr&: - ,LQT Aor A # MFP# AElian TololoancaNo ratings yet
- Memoria Autobiografica Suntem Dependenti de Trecut?: Dragos Cirneci Universitatea Spiru Haret BucurestiDocument53 pagesMemoria Autobiografica Suntem Dependenti de Trecut?: Dragos Cirneci Universitatea Spiru Haret Bucurestiflorina eNo ratings yet
- New Directions in Interpreting the Millon Clinical Multiaxial Inventory-III (MCMI-III)From EverandNew Directions in Interpreting the Millon Clinical Multiaxial Inventory-III (MCMI-III)No ratings yet
- Psychiatric DisordersDocument4 pagesPsychiatric DisordersarinahedianaNo ratings yet
- 07 Birney SternbergDocument71 pages07 Birney SternbergMariaIoanaTelecanNo ratings yet
- 18 241 1 PBDocument20 pages18 241 1 PBfordlee100% (1)
- Wechsler Adult Intelligence Scale - Wechsler Memory Scale DifferencDocument130 pagesWechsler Adult Intelligence Scale - Wechsler Memory Scale DifferencRaghuram MiryalaNo ratings yet
- Branson - 2019 - Vicarious Trauma, Themes in Research, and TerminolDocument9 pagesBranson - 2019 - Vicarious Trauma, Themes in Research, and TerminolheveanNo ratings yet
- A Way of Being, Bringing Mindfulness Into Individual Therapy PDFDocument14 pagesA Way of Being, Bringing Mindfulness Into Individual Therapy PDFJC Barrientos100% (1)
- ChestionarDocument10 pagesChestionarBiologie ProfesorNo ratings yet
- The Centrality of Control To Parenting and Its Effects, Barber, B. K., & Xia, M. (N.D.) - 61-87Document27 pagesThe Centrality of Control To Parenting and Its Effects, Barber, B. K., & Xia, M. (N.D.) - 61-87caballeroNo ratings yet
- PBQ-SF - Structure of The PBQ-SF - Smallest Space Analyses 2012Document7 pagesPBQ-SF - Structure of The PBQ-SF - Smallest Space Analyses 2012DoniLeiteNo ratings yet
- Evaluarea Personalitãtii Din Perspectiva Modelului Big Five. Date Privindad Aptarea Chestionarului IPIP-50 Pe Un Esantion de Studenti RomâniDocument18 pagesEvaluarea Personalitãtii Din Perspectiva Modelului Big Five. Date Privindad Aptarea Chestionarului IPIP-50 Pe Un Esantion de Studenti RomâniamnessiaNo ratings yet
- Kolb Whishaw 2014 Origins of Brain and Behavior PDFDocument31 pagesKolb Whishaw 2014 Origins of Brain and Behavior PDFVINZ VOGUENo ratings yet
- Inscopix NVista Product BrochureDocument8 pagesInscopix NVista Product BrochureSEO NeuroscienceNo ratings yet
- Instructions For Scoring CATS: Scale Child Range Clinical Cut-OffDocument2 pagesInstructions For Scoring CATS: Scale Child Range Clinical Cut-OffNor Khadijah AbdelkrimNo ratings yet
- Consiliere PsihologicaDocument168 pagesConsiliere PsihologicaAdriana BorzaNo ratings yet
- Workshopuri SibiuDocument21 pagesWorkshopuri SibiuDyana AnghelNo ratings yet
- Whole Brain Functional Training Using Multivariate Proportional Z-ScoresDocument47 pagesWhole Brain Functional Training Using Multivariate Proportional Z-ScoresAdriano GodoyNo ratings yet
- Emotion Regulation StrategiesDocument4 pagesEmotion Regulation StrategiesRăzvan-Andrei ZaicaNo ratings yet
- WIPPF Profile in Anxiety DisordersDocument10 pagesWIPPF Profile in Anxiety DisordersDelia CormosNo ratings yet
- A M Guidebook RomanianDocument36 pagesA M Guidebook RomanianScm Corina MariaNo ratings yet
- Mihaela Minulescu psychology evaluation documentsDocument2 pagesMihaela Minulescu psychology evaluation documentsdownloadfisierNo ratings yet
- Why Increases in Adolescent Depression May Be Linked To The Technological EnvironmentDocument6 pagesWhy Increases in Adolescent Depression May Be Linked To The Technological EnvironmentNova SafitriNo ratings yet
- Partea IIDocument96 pagesPartea IIChiorean DafinaNo ratings yet
- Parenting Stress, Child Adjustment, and Future Research QuestionsDocument19 pagesParenting Stress, Child Adjustment, and Future Research QuestionsBianca SerafincianuNo ratings yet
- Researchcentral: Despre Researchcentral Echipa Lista Testelor Recomandari de Utilizare Participa ContactDocument2 pagesResearchcentral: Despre Researchcentral Echipa Lista Testelor Recomandari de Utilizare Participa ContactDorin TriffNo ratings yet
- Articol Lavinia Tanculescu - Plesea - RSPH - Sept2019Document10 pagesArticol Lavinia Tanculescu - Plesea - RSPH - Sept2019Lavinia TanculescuNo ratings yet
- PANSSDocument2 pagesPANSSAgli AdhityaNo ratings yet
- Sacs Sub ScaleDocument2 pagesSacs Sub Scaleastridich100% (1)
- The Relationship Between Perfectionism, Stress and Burnout in Clinical PsychologistsDocument13 pagesThe Relationship Between Perfectionism, Stress and Burnout in Clinical PsychologistsVinícius SoaresNo ratings yet
- APA DSM 5 Substance Use DisorderDocument2 pagesAPA DSM 5 Substance Use DisorderRicardo Antonio Rivas SánchezNo ratings yet
- Aro Village SystemDocument5 pagesAro Village SystemObehi EromoseleNo ratings yet
- Joseph Grossman, Jewish Addiction Counselor, Intervention, Rehab Referrals, Jewish Addicts, OJA, Outreach For Jewish Addicts, Ami Magazine ArticleDocument5 pagesJoseph Grossman, Jewish Addiction Counselor, Intervention, Rehab Referrals, Jewish Addicts, OJA, Outreach For Jewish Addicts, Ami Magazine ArticleJoeGroNo ratings yet
- Atasament Si AnxietateDocument20 pagesAtasament Si AnxietateIon GheorgheNo ratings yet
- Psihologia PozitivaDocument10 pagesPsihologia PozitivaClaudiaClotanNo ratings yet
- רשות- Ch. 13 from Reynolds 2021- Mastering modern psychological testing 2ed.Document46 pagesרשות- Ch. 13 from Reynolds 2021- Mastering modern psychological testing 2ed.Casey KravitzNo ratings yet
- NottinghamDocument3 pagesNottinghamMental SidNo ratings yet
- Loneliness ScaleDocument14 pagesLoneliness Scalesandesh bhaisareNo ratings yet
- Offenders With Complex Needs - Analysis ReportDocument76 pagesOffenders With Complex Needs - Analysis ReportTONICNo ratings yet
- Todor Otilia 1Document6 pagesTodor Otilia 1pallavi gaikwadNo ratings yet
- Boala PakinsonDocument120 pagesBoala PakinsonMadalina CordonasuNo ratings yet
- Kaplan - Sadocks Synopsis of Psychiatry, 11th Edition-318-323Document6 pagesKaplan - Sadocks Synopsis of Psychiatry, 11th Edition-318-323nurmaulida568No ratings yet
- Psychology Study Guide, 8th EditionDocument476 pagesPsychology Study Guide, 8th EditionJoseph Jones67% (3)
- The Use and Misuse of Psychiatric Drugs: An Evidence-Based CritiqueFrom EverandThe Use and Misuse of Psychiatric Drugs: An Evidence-Based CritiqueNo ratings yet
- EI CentersDocument1 pageEI CentersFiorellaBeatrizNo ratings yet
- Milestone Moments GuideDocument60 pagesMilestone Moments GuideFiorellaBeatrizNo ratings yet
- QIToolkit ProjectPlanningFormDocument4 pagesQIToolkit ProjectPlanningFormFiorellaBeatrizNo ratings yet
- Chairman Rounds: Medicine I Jesse Lester, Kannan Samy, Matt Skomorowski, Dan VerrillDocument25 pagesChairman Rounds: Medicine I Jesse Lester, Kannan Samy, Matt Skomorowski, Dan VerrillFiorellaBeatrizNo ratings yet
- Sample Case PresentaionDocument10 pagesSample Case PresentaionFiorellaBeatrizNo ratings yet
- CatchresidentcallDocument5 pagesCatchresidentcallFiorellaBeatrizNo ratings yet
- Catch Application SampleDocument2 pagesCatch Application SampleFiorellaBeatrizNo ratings yet
- Physician Guide to Prescription WritingDocument36 pagesPhysician Guide to Prescription WritingFiorellaBeatrizNo ratings yet
- CS2 Blank Patient NoteDocument5 pagesCS2 Blank Patient NoteFiorellaBeatrizNo ratings yet
- Introduction To Laboratory Tests Handout VersionDocument58 pagesIntroduction To Laboratory Tests Handout VersionFiorellaBeatrizNo ratings yet
- Sample Case PresentaionDocument10 pagesSample Case PresentaionFiorellaBeatrizNo ratings yet
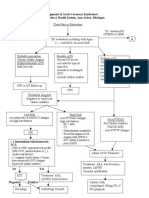
- Management of Acute Coronary Syndromes St. Joseph Mercy Health System, Ann Arbor, MichiganDocument2 pagesManagement of Acute Coronary Syndromes St. Joseph Mercy Health System, Ann Arbor, MichiganFiorellaBeatrizNo ratings yet
- Medscape Family MedDocument23 pagesMedscape Family MedRobert JenNo ratings yet
- Study Guide For OBGYNDocument34 pagesStudy Guide For OBGYNFiorellaBeatriz100% (1)
- Chairman Rounds: Medicine I Jesse Lester, Kannan Samy, Matt Skomorowski, Dan VerrillDocument25 pagesChairman Rounds: Medicine I Jesse Lester, Kannan Samy, Matt Skomorowski, Dan VerrillFiorellaBeatrizNo ratings yet
- Resilience Ace Screening ParentsDocument4 pagesResilience Ace Screening ParentsFiorellaBeatrizNo ratings yet
- Weekly AssignmentDocument3 pagesWeekly AssignmentFiorellaBeatrizNo ratings yet
- OB-GYN - Shelf Review NotesDocument47 pagesOB-GYN - Shelf Review NotesJackJoseph95% (19)
- CYW ACEQ UserGuideDocument21 pagesCYW ACEQ UserGuideFiorellaBeatrizNo ratings yet
- FMStudent OME VideoGuideForFMDocument4 pagesFMStudent OME VideoGuideForFMFiorellaBeatriz100% (1)
- Developmental Milestones For PDFDocument1 pageDevelopmental Milestones For PDFFiorellaBeatrizNo ratings yet
- Resistant HTNDocument7 pagesResistant HTNFiorellaBeatrizNo ratings yet
- Table9-3 Reflexes PDFDocument2 pagesTable9-3 Reflexes PDFFiorellaBeatrizNo ratings yet
- Ped Intake Form PDFDocument4 pagesPed Intake Form PDFFiorellaBeatrizNo ratings yet
- American Academy of Pediatrics and American Academy of Family PhysiciansDocument17 pagesAmerican Academy of Pediatrics and American Academy of Family PhysiciansFiorellaBeatrizNo ratings yet
- Denver II Test Form PDFDocument2 pagesDenver II Test Form PDFFiorellaBeatriz100% (3)
- 552.full DisparitiesDocument4 pages552.full DisparitiesFiorellaBeatrizNo ratings yet
- Russell Lancet Diabetes1Document11 pagesRussell Lancet Diabetes1FiorellaBeatrizNo ratings yet
- Organizational Behavior: Chapter 12: Basic Approaches To LeadershipDocument9 pagesOrganizational Behavior: Chapter 12: Basic Approaches To LeadershipTonmoy ParthoNo ratings yet
- Math Project ProposalDocument4 pagesMath Project ProposalNapoleon Agbing85% (26)
- Subfiels of LinguisticsDocument1 pageSubfiels of LinguisticsZoePhilipNo ratings yet
- LP - Math PrimaryDocument5 pagesLP - Math Primarykishore84No ratings yet
- Self-Control Model of DepressionDocument18 pagesSelf-Control Model of Depressionxdroka100% (2)
- Delisle, G. (1991) - A Gestalt Perspective of Personality DisordersDocument10 pagesDelisle, G. (1991) - A Gestalt Perspective of Personality DisordersAnte Župić100% (1)
- Teaching Learning ProcessDocument17 pagesTeaching Learning ProcessTUSHTI SHARMA100% (48)
- Characteristics of IODocument5 pagesCharacteristics of IOLynzae100% (2)
- IPCRF PPST RPMS FOR T1 3 - 2021 2022 v2.0Document56 pagesIPCRF PPST RPMS FOR T1 3 - 2021 2022 v2.0Krystal Antonio0% (2)
- Math Context For Learning (Task 4)Document3 pagesMath Context For Learning (Task 4)api-242665012100% (2)
- Instructional Strategies A-ZDocument78 pagesInstructional Strategies A-ZAlkaNo ratings yet
- Grade 7 Daily Lesson Log: G7 SPFLDocument3 pagesGrade 7 Daily Lesson Log: G7 SPFLzarriane AbordoNo ratings yet
- Edu480 Chapter 1Document16 pagesEdu480 Chapter 1Solehin Ab RahmanNo ratings yet
- Training Program: Evaluation of Trainees Expectation and ExperienceDocument13 pagesTraining Program: Evaluation of Trainees Expectation and ExperienceKaruna SoniNo ratings yet
- Interview Assessment FormDocument1 pageInterview Assessment FormCathleya Marie CoNo ratings yet
- Talent and Talent Management Insights: NHS Leadership Academy 201 5Document22 pagesTalent and Talent Management Insights: NHS Leadership Academy 201 5Alina IonelaNo ratings yet
- 3rd International Conference On Business Management ICBM 2018 PDFDocument420 pages3rd International Conference On Business Management ICBM 2018 PDFkripal shresthaNo ratings yet
- Dyadic Coping and Relationship Satisfaction A Meta-AnalysisDocument19 pagesDyadic Coping and Relationship Satisfaction A Meta-AnalysismerveNo ratings yet
- Management of Co-Curricular ActivitiesDocument32 pagesManagement of Co-Curricular Activitiesghs januwalaNo ratings yet
- Schyns & Schilling - A Meta-Analysis of Destructive Leadership A Its OutcomesDocument21 pagesSchyns & Schilling - A Meta-Analysis of Destructive Leadership A Its OutcomesVio Neagu100% (1)
- PSC 148 FinaDocument4 pagesPSC 148 Finaapi-579176860No ratings yet
- Moos Rubric CritthinkingDocument5 pagesMoos Rubric CritthinkingjalalNo ratings yet
- Inquiry-Based Teaching Strategies for Social StudiesDocument5 pagesInquiry-Based Teaching Strategies for Social StudiesCYRIL COSCOSNo ratings yet
- DLL FCPDocument2 pagesDLL FCPCece GregorioNo ratings yet
- Final Math533lesson DistributivepropertyweeblyDocument6 pagesFinal Math533lesson Distributivepropertyweeblyapi-256388918No ratings yet
- Sample Teacher Improvement Plan (Tip) /teacher Development PlanDocument2 pagesSample Teacher Improvement Plan (Tip) /teacher Development PlanJuliet Dela Cerna100% (1)
- 2 Principles of LearningDocument25 pages2 Principles of LearningAnjanette Velasquez100% (3)
- Soft Skills - Problem Solving SkillsDocument9 pagesSoft Skills - Problem Solving SkillsEida HidayahNo ratings yet
- Action Research Number Sense Math ConfidenceDocument11 pagesAction Research Number Sense Math Confidenceapi-545847738No ratings yet
- Camarines Norte State College: Management of Stress Amidst COVID-19 Uncertainties: Mental Health Advocacy Virtual WebinarDocument2 pagesCamarines Norte State College: Management of Stress Amidst COVID-19 Uncertainties: Mental Health Advocacy Virtual WebinarMarlon LorenzoNo ratings yet