You might also like
- Bates Chapter 8 Lung and ThoraxDocument15 pagesBates Chapter 8 Lung and ThoraxAdrian CaballesNo ratings yet
- Bioethical, Legal IssuesDocument6 pagesBioethical, Legal IssuesAlyxen PelingenNo ratings yet
- Captain of The Ship DoctrineDocument3 pagesCaptain of The Ship DoctrineAllison CuevasNo ratings yet
- Doctrines Applied in Medical Malpractice CasesDocument20 pagesDoctrines Applied in Medical Malpractice CasesMJ CarreonNo ratings yet
- Banzuela PhilHealth Handout 2014Document17 pagesBanzuela PhilHealth Handout 2014Wendy LucasNo ratings yet
- Med Juris FinalDocument17 pagesMed Juris FinalMarivicTalomaNo ratings yet
- Medical JurisprudenceDocument5 pagesMedical JurisprudenceMujeeb ChoudharyNo ratings yet
- Pedia QuizesDocument19 pagesPedia QuizesPraneeth PaletiNo ratings yet
- Medical JurisprudenceDocument4 pagesMedical JurisprudenceFLMNo ratings yet
- Global Leprosy StrategyDocument36 pagesGlobal Leprosy StrategyBlue PielagoNo ratings yet
- Clinical Pathology Introductory LectureDocument14 pagesClinical Pathology Introductory Lecture11101955100% (1)
- Medical JurisprudenceDocument60 pagesMedical JurisprudenceIvan LeeNo ratings yet
- PEDIA Clerks Revalida Review 2023Document106 pagesPEDIA Clerks Revalida Review 2023Raven EvangelistaNo ratings yet
- Qbank Vol 2 Clinical SciencesDocument227 pagesQbank Vol 2 Clinical SciencesGRATER ZNo ratings yet
- Dermoid CystDocument29 pagesDermoid CystAlik ChuaNo ratings yet
- Basic Education - Asinan Campus Columban College, Inc. Olongapo CityDocument38 pagesBasic Education - Asinan Campus Columban College, Inc. Olongapo CityKaye RegenciaNo ratings yet
- RA 7875 Amended by RA 11223 Universal Health Care ActDocument21 pagesRA 7875 Amended by RA 11223 Universal Health Care ActChristopher AdvinculaNo ratings yet
- Medical Jurisprudence GuideDocument13 pagesMedical Jurisprudence GuideSev SevaarNo ratings yet
- Arthritis Case Presentation - Dr. KlaesDocument27 pagesArthritis Case Presentation - Dr. KlaesShanti VennamNo ratings yet
- MechanicalDocument3 pagesMechanicalRoscelie KhoNo ratings yet
- Post Test Patho 1Document3 pagesPost Test Patho 1Kristine MangasepNo ratings yet
- DiverticulitisDocument15 pagesDiverticulitisElisabeth MelisaNo ratings yet
- ZZZZZZZDocument34 pagesZZZZZZZmikeNo ratings yet
- Leopando Hospice-Palliative3Document2 pagesLeopando Hospice-Palliative3Judy Ignacio EclarinoNo ratings yet
- Section 6. Time Limit For Trial. - XXX in No Case Shall TheDocument3 pagesSection 6. Time Limit For Trial. - XXX in No Case Shall TheClau ArrabisNo ratings yet
- SCREEMDocument2 pagesSCREEMDranreb Berylle MasangkayNo ratings yet
- Generics Act ReportDocument18 pagesGenerics Act ReportShiela Mae LopezNo ratings yet
- NCMA 219 RUBRICS Administering Blood TransfusionDocument2 pagesNCMA 219 RUBRICS Administering Blood Transfusioncaitie miracleNo ratings yet
- Natividad Agana CaseDocument14 pagesNatividad Agana CaseChuckieBoy Torre100% (1)
- Portal Hypertension - A Case ReportDocument65 pagesPortal Hypertension - A Case ReportTEAM K 1920No ratings yet
- Family Medicine COPCDocument20 pagesFamily Medicine COPCrachellesliedeleonNo ratings yet
- Practice of Medicine Medical Jurisprudence 67Document53 pagesPractice of Medicine Medical Jurisprudence 67Ulaysa100% (2)
- 1980 - Smilkstein's Cycle of Family FunctionDocument9 pages1980 - Smilkstein's Cycle of Family FunctionJoshua Benjamin Rocamora GrapaNo ratings yet
- Topnotch Waiver Oath and Checklist April 2015 PDFDocument2 pagesTopnotch Waiver Oath and Checklist April 2015 PDFRalph JuicoNo ratings yet
- Juris Legal Medicine SamplexDocument2 pagesJuris Legal Medicine SamplexLeomard SilverJoseph Centron Lim100% (1)
- Filipino Patient's Bill of RightsDocument1 pageFilipino Patient's Bill of RightsBernice Purugganan AresNo ratings yet
- Acute GastroenteritisDocument9 pagesAcute GastroenteritiscorsaruNo ratings yet
- Background of The Study ExampleDocument2 pagesBackground of The Study ExampleJohn Paulo RodriguezNo ratings yet
- REPUBLIC ACT No. 10932Document4 pagesREPUBLIC ACT No. 10932Marjorie LegaspiNo ratings yet
- CPG On CsomDocument8 pagesCPG On CsomRobert Ross DulayNo ratings yet
- Burn Ctu 312 - 2Document1 pageBurn Ctu 312 - 2Shaira Ann CalambaNo ratings yet
- Lecture Rickettsia Chlamydia, MycoplasmaDocument49 pagesLecture Rickettsia Chlamydia, MycoplasmaHabeeb Ali Baig100% (3)
- Donning and DoffingDocument10 pagesDonning and DoffingAla'a Emerald AguamNo ratings yet
- Nursing Malpractice and Negligence CasesDocument4 pagesNursing Malpractice and Negligence CasesGladys JhayeNo ratings yet
- Legal Medicine Questions 2Document17 pagesLegal Medicine Questions 2Luis PadillaNo ratings yet
- Ra 6138 PDF May 29 2012 10 40 Am 28kDocument2 pagesRa 6138 PDF May 29 2012 10 40 Am 28kShaira Mae CuevillasNo ratings yet
- Case Scenario (Lung Cancer)Document12 pagesCase Scenario (Lung Cancer)Mitzi CastuloNo ratings yet
- Biochem Finals Module 1 FinalsDocument10 pagesBiochem Finals Module 1 FinalsJeffrey RamosNo ratings yet
- 2021 Medjuris Board ReviewDocument32 pages2021 Medjuris Board ReviewLuis Padilla100% (1)
- Cerebrovascular DiseasesDocument16 pagesCerebrovascular DiseasesSopna ZenithNo ratings yet
- Chronic Myeloid LeukemiaDocument7 pagesChronic Myeloid LeukemiahemendreNo ratings yet
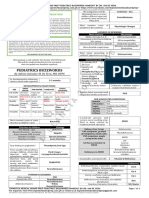
- 9 - Internal Medicine Buzzwords Handout Oct 2023 John Michael RuizDocument8 pages9 - Internal Medicine Buzzwords Handout Oct 2023 John Michael RuizJohn Michael RuizNo ratings yet
- Legal Medicine - Is A Branch of Medicine Which Deals With TheDocument8 pagesLegal Medicine - Is A Branch of Medicine Which Deals With TheJoselle ReyesNo ratings yet
- Finals Reviwer BB MtorgsethicsDocument236 pagesFinals Reviwer BB MtorgsethicsJames CabrigaNo ratings yet
- Pma Code of EthicsDocument40 pagesPma Code of Ethicsmaydansayco100% (1)
- EBM Self Instructional Manual 2008Document127 pagesEBM Self Instructional Manual 2008Adrian Oscar Z. Bacena100% (2)
- 5 - Legal Med Buzzwords Oct 2023 Jamaiyah H. Serad - Hadji OsopDocument10 pages5 - Legal Med Buzzwords Oct 2023 Jamaiyah H. Serad - Hadji OsopmikzhiNo ratings yet
- Finals Notes 34Document10 pagesFinals Notes 34Blaise VENo ratings yet
- SANCHEZ - Case Study Legal AspectDocument4 pagesSANCHEZ - Case Study Legal AspectCamille T. SanchezNo ratings yet
- Solidum Vs People of The PhilippinesDocument2 pagesSolidum Vs People of The PhilippinesAlyssa Denise A Averilla100% (1)
- Home Care: Fatima University Medical Center FMCH DepartmentDocument19 pagesHome Care: Fatima University Medical Center FMCH DepartmentIS99057100% (1)
- Coagulation DisordersDocument9 pagesCoagulation DisordersIS99057No ratings yet
- BronchiectasisDocument9 pagesBronchiectasisIS99057No ratings yet
- Anti Thrombotic Drugs and Transfusion MedicineDocument5 pagesAnti Thrombotic Drugs and Transfusion MedicineIS99057No ratings yet
- Hematology: Benign White Cell Disorder DR Thuy Feb 21 2017Document5 pagesHematology: Benign White Cell Disorder DR Thuy Feb 21 2017IS99057No ratings yet
- Orthotics and Assistive Devices OrthoticsDocument3 pagesOrthotics and Assistive Devices OrthoticsIS99057No ratings yet
- Dopamine Receptor AntagonistsDocument25 pagesDopamine Receptor AntagonistsIS99057No ratings yet
- Psychopharmacology: Rainier B. Umali, M.DDocument198 pagesPsychopharmacology: Rainier B. Umali, M.DIS99057No ratings yet
- Appnut Finals (No Aging)Document12 pagesAppnut Finals (No Aging)IS99057No ratings yet
- Observational: Observing Participants. You CannotDocument6 pagesObservational: Observing Participants. You CannotIS99057No ratings yet
- Co-Receptor: Cell Surface Receptor LigandDocument11 pagesCo-Receptor: Cell Surface Receptor LigandIS99057No ratings yet
- Legal Med - Ratio CompleteDocument25 pagesLegal Med - Ratio CompleteIS99057No ratings yet
- Epidemiologic Studies TransDocument5 pagesEpidemiologic Studies TransIS99057No ratings yet
- Pigments (Residual Autophagic Bodies)Document2 pagesPigments (Residual Autophagic Bodies)IS99057No ratings yet
- Neoplasia I - RecordingDocument6 pagesNeoplasia I - RecordingIS99057No ratings yet
- Doctrine of The MeanDocument2 pagesDoctrine of The MeansteveNo ratings yet
- Bush Sr. and Bill ClintonDocument17 pagesBush Sr. and Bill ClintonTimothy100% (2)
- SOP (Client Arrival) - 2Document2 pagesSOP (Client Arrival) - 2arishinewatiaNo ratings yet
- Police PatrolDocument130 pagesPolice PatrolEcho EchoNo ratings yet
- Navig8 Almandine - Inv No 2019-002 - Santa Barbara Invoice + Voucher PDFDocument2 pagesNavig8 Almandine - Inv No 2019-002 - Santa Barbara Invoice + Voucher PDFAnonymous MoQ28DEBPNo ratings yet
- IPM 2022 - Global CompendiumDocument83 pagesIPM 2022 - Global Compendiumdanielle evansNo ratings yet
- Scripbox Reg FormDocument6 pagesScripbox Reg FormRohan SinghNo ratings yet
- Dust DevilsDocument6 pagesDust DevilsRobNo ratings yet
- SBD Apparel Limited v. A7 Fitness - ComplaintDocument22 pagesSBD Apparel Limited v. A7 Fitness - ComplaintSarah Burstein100% (1)
- In The Court of Appeal of The Republic of Singapore: (2020) SGCA 06Document33 pagesIn The Court of Appeal of The Republic of Singapore: (2020) SGCA 06Faizan BhatNo ratings yet
- Lift Plan v2Document3 pagesLift Plan v2Hussain YahyaNo ratings yet
- Role of Ethics in Corporate GovernanceDocument11 pagesRole of Ethics in Corporate GovernancepranjalNo ratings yet
- Ellen G. White's Writings - Their Role and FunctionDocument108 pagesEllen G. White's Writings - Their Role and FunctionAntonio BernardNo ratings yet
- Bank File FormatDocument2 pagesBank File Formatpmenocha8799100% (1)
- AKSI Annual Report 2018Document126 pagesAKSI Annual Report 2018Rahmi AnggianiNo ratings yet
- Chapter C2 Formation of The Corporation Discussion QuestionsDocument16 pagesChapter C2 Formation of The Corporation Discussion QuestionsPennyW0% (1)
- Ifrs 9 Financial Instruments Using Models in Impairment - AshxDocument38 pagesIfrs 9 Financial Instruments Using Models in Impairment - Ashxwan nur anisahNo ratings yet
- Freedom - What Is Bible Freedom. What Does John 8:32 Promise?Document64 pagesFreedom - What Is Bible Freedom. What Does John 8:32 Promise?kgdieckNo ratings yet
- Miscellaneous Provisions: After Studying This Chapter, You Will Be Able ToDocument36 pagesMiscellaneous Provisions: After Studying This Chapter, You Will Be Able TofirastiNo ratings yet
- Quizzer Cash and Cash EquivalentsDocument10 pagesQuizzer Cash and Cash EquivalentsJoshua TorillaNo ratings yet
- Surety's Liability Under The Indian Contract Act, 1857Document15 pagesSurety's Liability Under The Indian Contract Act, 1857Joshu AbrahamNo ratings yet
- Spec Contract Appointment Letter.Document5 pagesSpec Contract Appointment Letter.zeeshan100% (1)
- Prophethood and Its Importance, The Life and Unique Qualities of Prophet Muhammad (Saw) CHP# 6Document28 pagesProphethood and Its Importance, The Life and Unique Qualities of Prophet Muhammad (Saw) CHP# 6Saman BaigNo ratings yet
- Instant Download Chemistry The Central Science Brown 11th Edition Test Bank PDF ScribdDocument32 pagesInstant Download Chemistry The Central Science Brown 11th Edition Test Bank PDF ScribdConsuelo Peral100% (13)
- No Shortchanging ActDocument11 pagesNo Shortchanging ActDesiree Ann GamboaNo ratings yet
- The Lion of Judah PDFDocument19 pagesThe Lion of Judah PDFMichael SympsonNo ratings yet
- Proposal For The Crestwood Plaza Redevelopment Area by UrbanStreet - Crestwood, MODocument52 pagesProposal For The Crestwood Plaza Redevelopment Area by UrbanStreet - Crestwood, MOnextSTL.comNo ratings yet
- Havells India LTD: Actuals Key Financials (Rs. in CRS.)Document159 pagesHavells India LTD: Actuals Key Financials (Rs. in CRS.)milan kakkadNo ratings yet
- Topic 3 - Overview: Licensing Exam Paper 1 Topic 3Document16 pagesTopic 3 - Overview: Licensing Exam Paper 1 Topic 3anonlukeNo ratings yet
- S.No Ward Zone License No License Validity Date Hawker Type Name Age Fathar/Husband NameDocument41 pagesS.No Ward Zone License No License Validity Date Hawker Type Name Age Fathar/Husband NameSandeep DhimanNo ratings yet