You might also like
- Legal Overview Restraint SchoolsDocument40 pagesLegal Overview Restraint SchoolsHWCLegalAlertNo ratings yet
- Legal Overview of Restraint in Juv. JusticeDocument37 pagesLegal Overview of Restraint in Juv. JusticeHWCLegalAlertNo ratings yet
- AASA: How Seclusion and Restraint Protects Students and School PersonnelDocument10 pagesAASA: How Seclusion and Restraint Protects Students and School PersonnelHWCLegalAlertNo ratings yet
- LGBT EssayDocument5 pagesLGBT EssayAhWeiNo ratings yet
- Employment Contract Template 1414717815774Document5 pagesEmployment Contract Template 1414717815774Santee HaylesNo ratings yet
- Petition To Initiate Rule Making To Reschedule MarijuanaDocument6 pagesPetition To Initiate Rule Making To Reschedule MarijuanaJohnNo ratings yet
- Legal Aspects of Healthcare Administration AssignmentDocument7 pagesLegal Aspects of Healthcare Administration Assignmentjossy MulingeNo ratings yet
- Informed Consent SampleDocument7 pagesInformed Consent SampleArjuna BuduhNo ratings yet
- Republic Act No. 9484Document7 pagesRepublic Act No. 9484Jay-arr ValdezNo ratings yet
- Oath On PrivacyDocument1 pageOath On Privacydivina aquinoNo ratings yet
- Oplan Tokhang Case StudyDocument4 pagesOplan Tokhang Case StudyJayson OliveraNo ratings yet
- Required consent and documents for child adoptionDocument2 pagesRequired consent and documents for child adoptionKarla EspinosaNo ratings yet
- Dole sets guidelines for K-12 work immersion programDocument6 pagesDole sets guidelines for K-12 work immersion programErika VeepieNo ratings yet
- Election CasesDocument126 pagesElection CasesApril Joy Matudio Rabang - BaylosisNo ratings yet
- Lecture Vawc Rape BullyingDocument40 pagesLecture Vawc Rape BullyingWcpd Baggao PSNo ratings yet
- Eligibility To Adopt: Adoption Process by Filing Form I-800A. Do Not Accept Any Adoption Placement Before USCIS HasDocument17 pagesEligibility To Adopt: Adoption Process by Filing Form I-800A. Do Not Accept Any Adoption Placement Before USCIS HasNadineNo ratings yet
- Principles of InterviewingDocument2 pagesPrinciples of Interviewingnarjis batoolNo ratings yet
- Overuse of Pretrial Detention in Tension With Judicial and Prison Reforms in The Dominican RepublicDocument25 pagesOveruse of Pretrial Detention in Tension With Judicial and Prison Reforms in The Dominican RepublicYunior Andrés Castillo SilverioNo ratings yet
- Negligence of DutyDocument8 pagesNegligence of DutyChristopher LaneNo ratings yet
- ADMINISTRATIVE ORDER Excavation PermitDocument2 pagesADMINISTRATIVE ORDER Excavation PermitDeil L. NaveaNo ratings yet
- Correction Pillar 2Document46 pagesCorrection Pillar 2Harren SajaNo ratings yet
- Natural Resources and Environment Law SyllabusDocument5 pagesNatural Resources and Environment Law SyllabusMel Joshua MajestradoNo ratings yet
- An Overview On The Juvenile Justice System in The PhilippinesDocument10 pagesAn Overview On The Juvenile Justice System in The PhilippinesJake CopradeNo ratings yet
- Voluntary Post-Adoption Contact AgreementsDocument4 pagesVoluntary Post-Adoption Contact AgreementsMetz Lewis Brodman Must O'Keefe LLCNo ratings yet
- Ra 9344Document36 pagesRa 9344Rafael SaturnoNo ratings yet
- A. Demand LetterDocument2 pagesA. Demand LetterCzarina BantayNo ratings yet
- The Filipino School Counselor As Practicum Supervisee - Perceptions On Practicum Supervision in CounselingDocument12 pagesThe Filipino School Counselor As Practicum Supervisee - Perceptions On Practicum Supervision in CounselingYanurzkie MallorcaNo ratings yet
- Criminal Justice Trends Paper Analyzes Past, Present and Future Trends Impacting Corrections/TITLEDocument9 pagesCriminal Justice Trends Paper Analyzes Past, Present and Future Trends Impacting Corrections/TITLErosa martinezNo ratings yet
- Comprehensive Dangerous Drugs Act of 2002, Republic Act No. 9165 - PhilippinesDocument62 pagesComprehensive Dangerous Drugs Act of 2002, Republic Act No. 9165 - PhilippinesRam Francis ClareNo ratings yet
- PNPDocument2 pagesPNPKitaotao MPS PnpNo ratings yet
- The Revised Forestry Code Power PointDocument15 pagesThe Revised Forestry Code Power PointCglu NemNo ratings yet
- Ra 7610Document57 pagesRa 7610Jan Hyacinth GondaNo ratings yet
- Complaint Affidavit Case 2Document3 pagesComplaint Affidavit Case 2Carlyn Belle de GuzmanNo ratings yet
- Joint Affidavit of Two Disinterested Witnesses Attesting Oneness of NameDocument1 pageJoint Affidavit of Two Disinterested Witnesses Attesting Oneness of NameNoel Ephraim AntiguaNo ratings yet
- Philippines PDFDocument49 pagesPhilippines PDFMau AntallanNo ratings yet
- Affidavit of Admission of PaternityDocument1 pageAffidavit of Admission of PaternitykadjubalandayNo ratings yet
- Magna Carta of Women Rights Law SummaryDocument5 pagesMagna Carta of Women Rights Law SummaryAileen CapiliNo ratings yet
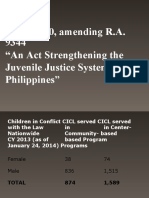
- R.A. 10630, Amending R.A. 9344 "An Act Strengthening The Juvenile Justice System in The PhilippinesDocument16 pagesR.A. 10630, Amending R.A. 9344 "An Act Strengthening The Juvenile Justice System in The PhilippinesNur SanaaniNo ratings yet
- Letter of Commendation To Sheila BayanganDocument1 pageLetter of Commendation To Sheila BayanganVev'z Dangpason BalawanNo ratings yet
- Cayetano Vs MonsodDocument20 pagesCayetano Vs MonsodKem100% (1)
- ADGE SyllabusDocument8 pagesADGE SyllabusHersie Bunda100% (1)
- Pretrial Intervention Program PTIDocument6 pagesPretrial Intervention Program PTIKenneth Vercammen, Esq.100% (1)
- Ra 11463Document15 pagesRa 11463Elizabeth DullaNo ratings yet
- Civil Service Commission Res. No. 01-0940Document16 pagesCivil Service Commission Res. No. 01-0940JaneGonzalezMartinez100% (1)
- RA 9165: Comprehensive Dangerous Drugs ActDocument52 pagesRA 9165: Comprehensive Dangerous Drugs ActCabagan IsabelaNo ratings yet
- Reduction (NHTS-PR), An Information Management System That Employs Geographic Targeting, HouseholdDocument3 pagesReduction (NHTS-PR), An Information Management System That Employs Geographic Targeting, HouseholdLloyd Ian FongfarNo ratings yet
- Background Investigation FormDocument2 pagesBackground Investigation FormOcsi YeahNo ratings yet
- Employee Benefits in The PhilippinesDocument3 pagesEmployee Benefits in The PhilippinesRheii SparksNo ratings yet
- Ra 9184Document24 pagesRa 9184Fannie GailNo ratings yet
- REPUBLIC ACT 11596 - An Act Prohibiting Child MarriageDocument20 pagesREPUBLIC ACT 11596 - An Act Prohibiting Child MarriageRic VinceNo ratings yet
- The Person To Be Adopted Is:: The Qualifications of The AdopterDocument1 pageThe Person To Be Adopted Is:: The Qualifications of The AdopterKris CalabiaNo ratings yet
- Syllabus 2022 (Nat Res Env Law)Document17 pagesSyllabus 2022 (Nat Res Env Law)Frances Rexanne AmbitaNo ratings yet
- Digested Case 3Document19 pagesDigested Case 3bingadanzaNo ratings yet
- Presumption of InnocenceDocument6 pagesPresumption of InnocenceAlok BagriNo ratings yet
- SPECIAL POWER OF ATTORNEY Jose GIORGIO BORRES1Document1 pageSPECIAL POWER OF ATTORNEY Jose GIORGIO BORRES1Hersie BundaNo ratings yet
- BJMP Provident Fund FormDocument1 pageBJMP Provident Fund FormGeneris SuiNo ratings yet
- Child AdoptionDocument21 pagesChild AdoptionMohamad Zafri MahmudNo ratings yet
- University of The Philippines College of LawDocument5 pagesUniversity of The Philippines College of Lawrm2803No ratings yet
- RH LawDocument15 pagesRH LawFrost RideNo ratings yet
- Critique On The Responsible ParenthoodDocument18 pagesCritique On The Responsible ParenthoodAbdulhakim BasirNo ratings yet
- In Defense ofDocument9 pagesIn Defense ofHWCLegalAlertNo ratings yet
- New York Report On Violence in SchoolsDocument2 pagesNew York Report On Violence in SchoolsHWCLegalAlertNo ratings yet
- Congressional Research Service: Legal IssuesDocument11 pagesCongressional Research Service: Legal IssuesHWCLegalAlertNo ratings yet
- Georgia Rule On Restraint & Seclusion v. Right To Defend Oneself and OthersDocument3 pagesGeorgia Rule On Restraint & Seclusion v. Right To Defend Oneself and OthersHWCLegalAlertNo ratings yet
- SDS (Safety Data Sheet) For LRV Vehicle Cleaning and OMSF Facilities Expired SheetsDocument4 pagesSDS (Safety Data Sheet) For LRV Vehicle Cleaning and OMSF Facilities Expired SheetsmilandivacNo ratings yet
- Renal Tumor and Polycystic Kidney DiseaseDocument6 pagesRenal Tumor and Polycystic Kidney DiseaseMahdawwNo ratings yet
- FinalstatementofintentDocument1 pageFinalstatementofintentapi-546274167No ratings yet
- Covid Patients2022Document221 pagesCovid Patients2022Sample BakeshopNo ratings yet
- CHD With NCPDocument10 pagesCHD With NCPJohanna Kirsten F. DaguioNo ratings yet
- Welcome Plan Welcome CorpsDocument10 pagesWelcome Plan Welcome Corpscs310201No ratings yet
- Kerry Bone Covid 19 PresentationDocument27 pagesKerry Bone Covid 19 PresentationLukasNo ratings yet
- Brand Plan - SingulairDocument11 pagesBrand Plan - Singulairshashank100% (2)
- Contraceptive MethodDocument17 pagesContraceptive MethodKarina Puspita SariNo ratings yet
- Trodat 7097 Fast Drying Flash Ink Black - 718327 - S - Eu - GBDocument11 pagesTrodat 7097 Fast Drying Flash Ink Black - 718327 - S - Eu - GBAshish TiwariNo ratings yet
- Experienced Power Plant Operator Seeking New OpportunityDocument4 pagesExperienced Power Plant Operator Seeking New OpportunityOwais Manzoor MalikNo ratings yet
- Peds - Research ArticleDocument2 pagesPeds - Research Articleapi-662219485No ratings yet
- Pulmonary and Respiratory Nursing Assessment GuideDocument48 pagesPulmonary and Respiratory Nursing Assessment GuideEmjay JapitanaNo ratings yet
- Lucrari Despre Calitatea VietiiDocument147 pagesLucrari Despre Calitatea VietiiCarmen MarianaNo ratings yet
- CH05: Understanding Family SystemsDocument3 pagesCH05: Understanding Family Systemskazelle GentallanNo ratings yet
- Medicine CaseDocument4 pagesMedicine CaseRoane RoblesNo ratings yet
- 2020 State of The Community: Transitional Aged YouthDocument82 pages2020 State of The Community: Transitional Aged YouthRoxanne ReevesNo ratings yet
- Dangers of Statin DrugsDocument17 pagesDangers of Statin Drugslijyonas100% (2)
- Aninditha. Buku Ajar Neurologi. Jakarta: Departemen Neurologi Fakultas Kedokteran Universitas Indonesia RS Cipto Mangunkusumo. 2017Document2 pagesAninditha. Buku Ajar Neurologi. Jakarta: Departemen Neurologi Fakultas Kedokteran Universitas Indonesia RS Cipto Mangunkusumo. 2017pelangiNo ratings yet
- What Is Functional HypertrophyDocument7 pagesWhat Is Functional Hypertrophynima_44No ratings yet
- Superfood Septembar 2019Document5 pagesSuperfood Septembar 2019Vladimir JovanovicNo ratings yet
- The House of Raminten English NewsDocument1 pageThe House of Raminten English Newsdelvino anantaNo ratings yet
- Health: Quarter 1 - Module 1Document11 pagesHealth: Quarter 1 - Module 1TIPAY, EMELIE L.No ratings yet
- Julian Villalba MD Biography IUATLDDocument2 pagesJulian Villalba MD Biography IUATLDJulian VillalbaNo ratings yet
- COVID-19 RNA-Based Vaccines and The Risk of Prion Disease 1503Document3 pagesCOVID-19 RNA-Based Vaccines and The Risk of Prion Disease 1503jermNo ratings yet
- Internal Stakeholders IssuesDocument14 pagesInternal Stakeholders IssuesdivyadeoNo ratings yet
- CURRENT STATUS OF CHILD HEALTH IN INDIA To Be PrintDocument6 pagesCURRENT STATUS OF CHILD HEALTH IN INDIA To Be Printprecillathoppil96% (24)
- Activity 1: Jevelav G. Tahadlangit BSCE-1A Oct. 22, 2020Document10 pagesActivity 1: Jevelav G. Tahadlangit BSCE-1A Oct. 22, 2020RJ TacataNo ratings yet
- JeremyDocument2 pagesJeremyManjuNo ratings yet
- First Aid Skill Retention of First Responders Within The WorkplaceDocument6 pagesFirst Aid Skill Retention of First Responders Within The WorkplaceYusri RamliNo ratings yet