You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Simple Tenses VerbsDocument69 pagesSimple Tenses VerbsRovi Chell100% (2)
- CFM-Barbara Norris CaseDocument10 pagesCFM-Barbara Norris CasevarunNo ratings yet
- When Your Baby Won't Eat - The New York TimesDocument14 pagesWhen Your Baby Won't Eat - The New York TimesEveraldo SkrockNo ratings yet
- Doctor FMT 2Document6 pagesDoctor FMT 2Thinnakorn ViroteNo ratings yet
- Medical BillingDocument16 pagesMedical BillingAbdul Gaffoor100% (5)
- An International Cohort Study of Cancer in Systemic Lupus ErythematosusDocument10 pagesAn International Cohort Study of Cancer in Systemic Lupus ErythematosusCristina TudorNo ratings yet
- Nursing Leadership and ManagementDocument48 pagesNursing Leadership and ManagementDarl DacdacNo ratings yet
- Scope of Nle1012Document334 pagesScope of Nle1012ericNo ratings yet
- Autopsy Manual 2014Document66 pagesAutopsy Manual 2014Steven ArroyoNo ratings yet
- HS CLT 3 TheRoleOfAPhlebotomistPowerPointDocument19 pagesHS CLT 3 TheRoleOfAPhlebotomistPowerPointtapan_tsgNo ratings yet
- Guidelines For The Management of Traumatic Dental Injuries - 1. Fractures and Luxations of Permanent TeethDocument11 pagesGuidelines For The Management of Traumatic Dental Injuries - 1. Fractures and Luxations of Permanent TeethArturo Trejo VeraNo ratings yet
- History of UphsDocument3 pagesHistory of UphsDIANE EDRANo ratings yet
- Malnutrition in Acute Care Patients: A Narrative Review: Cathy Kubrak, Louise JensenDocument19 pagesMalnutrition in Acute Care Patients: A Narrative Review: Cathy Kubrak, Louise JensenchanchandilNo ratings yet
- Clinical Experience With Affinity Pixie™ Oxygenation System in Paediatric and Infant PatientsDocument5 pagesClinical Experience With Affinity Pixie™ Oxygenation System in Paediatric and Infant Patientsفرید رضاییNo ratings yet
- Delhi DoctorsDocument165 pagesDelhi DoctorsDhruv Vasudeva50% (2)
- Keeping Preemies Warm, Breathing Well and EnergizedDocument8 pagesKeeping Preemies Warm, Breathing Well and Energizedindirinoor5No ratings yet
- Acalculous Cholecystitis Power PointDocument83 pagesAcalculous Cholecystitis Power PointClarissa Joy Jimenez100% (1)
- Annotated BibliographyDocument8 pagesAnnotated Bibliographyapi-495941898No ratings yet
- What Is A CataractDocument4 pagesWhat Is A CataractBhavin ShahNo ratings yet
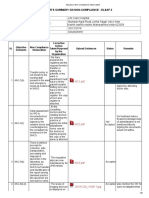
- Assessor Non Compliance ObservationDocument9 pagesAssessor Non Compliance ObservationSwati BajpaiNo ratings yet
- Assembly Bill No. 1340: Legislative Counsel's DigestDocument11 pagesAssembly Bill No. 1340: Legislative Counsel's DigestJon OrtizNo ratings yet
- Care for Patients as an LPN or LVNDocument10 pagesCare for Patients as an LPN or LVNSarah Vazquez FranNo ratings yet
- Blickley Blickley ResumeDocument2 pagesBlickley Blickley Resumeapi-450663790No ratings yet
- Pike County Coroner's Office: Terrell A. Moody, CoronerDocument4 pagesPike County Coroner's Office: Terrell A. Moody, CoronerClaireNo ratings yet
- Chapter 43 - Do The Surviving Sepsis Campaign Guidelines WorkDocument4 pagesChapter 43 - Do The Surviving Sepsis Campaign Guidelines WorkIkhlasul Amal WellNo ratings yet
- High Alert: MedicationsDocument25 pagesHigh Alert: MedicationsMarianne LayloNo ratings yet
- Patient Bill: Test Name Reporting Date & Time Rate SRDocument1 pagePatient Bill: Test Name Reporting Date & Time Rate SRShahab KhanNo ratings yet
- CASUMPANG v. CORTEJO: DOCTOR LIABLE FOR FAILING TO DIAGNOSE DENGUE FEVERDocument2 pagesCASUMPANG v. CORTEJO: DOCTOR LIABLE FOR FAILING TO DIAGNOSE DENGUE FEVERAlleine TupazNo ratings yet
- Mastering Health Economics with OUM Business SchoolDocument8 pagesMastering Health Economics with OUM Business SchoolMuhammad AliminNo ratings yet
- Hospice and Palliative Care in IndiaDocument9 pagesHospice and Palliative Care in IndiaArunpv001No ratings yet