You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Calculus of Finite Differences: Andreas KlappeneckerDocument30 pagesCalculus of Finite Differences: Andreas KlappeneckerSouvik RoyNo ratings yet
- Lecture No. 11Document15 pagesLecture No. 11Sayeda JabbinNo ratings yet
- Starex Is BTSDocument24 pagesStarex Is BTSKLNo ratings yet
- Dark Energy Survey DES CollaborationDocument38 pagesDark Energy Survey DES CollaborationgeorgcantorNo ratings yet
- Rewriting Snow White As A Powerful WomanDocument6 pagesRewriting Snow White As A Powerful WomanLaura RodriguezNo ratings yet
- Citing Correctly and Avoiding Plagiarism: MLA Format, 7th EditionDocument4 pagesCiting Correctly and Avoiding Plagiarism: MLA Format, 7th EditionDanish muinNo ratings yet
- Pitch AnythingDocument8 pagesPitch AnythingDoland drumb100% (1)
- Dashrath Nandan JAVA (Unit2) NotesDocument18 pagesDashrath Nandan JAVA (Unit2) NotesAbhinandan Singh RanaNo ratings yet
- NST 029Document123 pagesNST 029Riaz Ahmad BhattiNo ratings yet
- L Rexx PDFDocument9 pagesL Rexx PDFborisg3No ratings yet
- Analog Electronics-2 PDFDocument20 pagesAnalog Electronics-2 PDFAbhinav JangraNo ratings yet
- American J of Comm Psychol - 2023 - Palmer - Looted Artifacts and Museums Perpetuation of Imperialism and RacismDocument9 pagesAmerican J of Comm Psychol - 2023 - Palmer - Looted Artifacts and Museums Perpetuation of Imperialism and RacismeyeohneeduhNo ratings yet
- SAP Environment, Health, and Safety (EHS)Document13 pagesSAP Environment, Health, and Safety (EHS)SAFETY VOFPLNo ratings yet
- Project ProposalDocument2 pagesProject Proposalqueen malik80% (5)
- Sunrise - 12 AB-unlockedDocument81 pagesSunrise - 12 AB-unlockedMohamed Thanoon50% (2)
- Debate Lesson PlanDocument3 pagesDebate Lesson Planapi-280689729No ratings yet
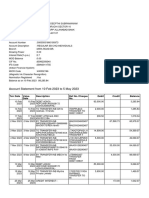
- Feb-May SBI StatementDocument2 pagesFeb-May SBI StatementAshutosh PandeyNo ratings yet
- Development of PBAT Based Bio Filler Masterbatch: A Scientific Research Proposal OnDocument15 pagesDevelopment of PBAT Based Bio Filler Masterbatch: A Scientific Research Proposal OnManmathNo ratings yet
- Ce Project 1Document7 pagesCe Project 1emmaNo ratings yet
- CBLM - Interpreting Technical DrawingDocument18 pagesCBLM - Interpreting Technical DrawingGlenn F. Salandanan89% (45)
- All Siae Skus: SF Product Name SIAE Product Code Descrip:on Availability Product Family Unit LIST Price ($)Document7 pagesAll Siae Skus: SF Product Name SIAE Product Code Descrip:on Availability Product Family Unit LIST Price ($)Emerson Mayon SanchezNo ratings yet
- B205A TMA Project Spring 2021 - UpdatedDocument6 pagesB205A TMA Project Spring 2021 - UpdatedIoan 23No ratings yet
- Approximate AnalysisDocument35 pagesApproximate AnalysisSyahir HamidonNo ratings yet
- Ugtt April May 2019 NewDocument48 pagesUgtt April May 2019 NewSuhas SNo ratings yet
- Ems Speed Sensor Com MotorDocument24 pagesEms Speed Sensor Com MotorKarina RickenNo ratings yet
- CSCI 123 - Final ExamDocument15 pagesCSCI 123 - Final ExamBrianYoungNo ratings yet
- AM-FM Reception TipsDocument3 pagesAM-FM Reception TipsKrishna Ghimire100% (1)
- Investigation of The Microstructures, Properties, and Toughening Mechanism of Polypropylene/calcium Carbonate Toughening Masterbatch CompositesDocument16 pagesInvestigation of The Microstructures, Properties, and Toughening Mechanism of Polypropylene/calcium Carbonate Toughening Masterbatch CompositesHatchi KouNo ratings yet
- Comsol - Guidelines For Modeling Rotating Machines in 3DDocument30 pagesComsol - Guidelines For Modeling Rotating Machines in 3DtiberiupazaraNo ratings yet
- Ojt Evaluation Forms (Supervised Industry Training) SampleDocument5 pagesOjt Evaluation Forms (Supervised Industry Training) SampleJayJay Jimenez100% (3)