You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Advertisement Analysis: Syntactic Devices in English MagazinesDocument5 pagesAdvertisement Analysis: Syntactic Devices in English MagazinesJASH MATHEWNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Assessment of The Use of National Standing Orders in The Treatment of Minor Ailments Among Community Health Practitioners in Ibadan MunicipalityDocument5 pagesAssessment of The Use of National Standing Orders in The Treatment of Minor Ailments Among Community Health Practitioners in Ibadan MunicipalityJASH MATHEWNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- F - DERIVATIONS ON BP-ALGEBRASDocument11 pagesF - DERIVATIONS ON BP-ALGEBRASJASH MATHEWNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Molecular Characterization of Extended-Spectrum BetaLactamase (ESBLs) Genes in Pseudomonas Aeruginosa From Pregnant Women Attending A Tertiary Health Care Centre in Makurdi, Central NigeriaDocument7 pagesMolecular Characterization of Extended-Spectrum BetaLactamase (ESBLs) Genes in Pseudomonas Aeruginosa From Pregnant Women Attending A Tertiary Health Care Centre in Makurdi, Central NigeriaJASH MATHEWNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Engaging Students Through Board Games: Measuring Its Effectiveness On Academic PerformanceDocument3 pagesEngaging Students Through Board Games: Measuring Its Effectiveness On Academic PerformanceJASH MATHEWNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Value Chain Analysis, at PT. Indofood CBP SuksesMakmurTbk (Noodle DivisionDocument5 pagesValue Chain Analysis, at PT. Indofood CBP SuksesMakmurTbk (Noodle DivisionJASH MATHEWNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Combining Ability Analysis of Early Maturing Maize (Zea Mays.l) Inbred Lines in Central Rift Valley of EthiopiaDocument13 pagesCombining Ability Analysis of Early Maturing Maize (Zea Mays.l) Inbred Lines in Central Rift Valley of EthiopiaJASH MATHEWNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Challenges and Opportunities of E-Payment in Ethiopia Banking Industry: With The Reference of Private Commercial BanksDocument8 pagesChallenges and Opportunities of E-Payment in Ethiopia Banking Industry: With The Reference of Private Commercial BanksJASH MATHEW100% (7)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Shift of Focalization in James Joyce's UlyssesDocument7 pagesThe Shift of Focalization in James Joyce's UlyssesJASH MATHEWNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Environmental Impact Assessment of Soil Quarrying From The Hills of Central Kerala, Southwest Coast of IndiaDocument8 pagesEnvironmental Impact Assessment of Soil Quarrying From The Hills of Central Kerala, Southwest Coast of IndiaJASH MATHEWNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Hegemonic Masculinity and Oppression of Women in CavedwellerDocument6 pagesHegemonic Masculinity and Oppression of Women in CavedwellerJASH MATHEWNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- A Study of Current Status Quo of English As A Second Language in India Study Done On West Bengal SchoolsDocument6 pagesA Study of Current Status Quo of English As A Second Language in India Study Done On West Bengal SchoolsJASH MATHEWNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Ijsrp p5656 PDFDocument8 pagesIjsrp p5656 PDFJASH MATHEWNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Puppy Socialization: What Is Puppy Socialization? Why Is Puppy Socialization Important?Document3 pagesPuppy Socialization: What Is Puppy Socialization? Why Is Puppy Socialization Important?Maria De Fátima BezerraNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Cursos de Italiano PDFDocument16 pagesCursos de Italiano PDFmagaly125No ratings yet
- Rubrics For Speaking CompetenceDocument1 pageRubrics For Speaking CompetenceAMELYN DACULANo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Programme Handbook 21-22 FinalDocument27 pagesProgramme Handbook 21-22 Final4wqzcq7p9xNo ratings yet
- The Role of A Leader in Stimulating Innovation in An OrganizationDocument18 pagesThe Role of A Leader in Stimulating Innovation in An OrganizationĐạt NguyễnNo ratings yet
- EN3NG03 Soft Skills IDocument2 pagesEN3NG03 Soft Skills IsourabhNo ratings yet
- Queens Alumni Review 2012 - Spotlight: Bruce AlexanderDocument2 pagesQueens Alumni Review 2012 - Spotlight: Bruce Alexanderalpha_abebeNo ratings yet
- 1 Full List of LkoDocument6 pages1 Full List of Lkomohd yusuf ansariNo ratings yet
- Assignment 1 Lesson Plan and CritiqueDocument12 pagesAssignment 1 Lesson Plan and Critiqueapi-327519956No ratings yet
- Energy ClubDocument7 pagesEnergy ClubAdesh MidhaNo ratings yet
- The Effects of Vote Buying in Lanao Del Sur For This Coming Election 2022Document17 pagesThe Effects of Vote Buying in Lanao Del Sur For This Coming Election 2022Gerryanna MagbitangNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- An Assignment On Checklist: Submitted To:-Submitted By: - Divya MSC NSG 1 YearDocument4 pagesAn Assignment On Checklist: Submitted To:-Submitted By: - Divya MSC NSG 1 YearNehaNo ratings yet
- Iss Clark Kozma DebateDocument8 pagesIss Clark Kozma Debateapi-357361009100% (1)
- Pulpitis ReversiibleDocument7 pagesPulpitis ReversiibleAlsilaNo ratings yet
- Senior Scientist Microbiologist in Boston MA Resume Adhar MannaDocument2 pagesSenior Scientist Microbiologist in Boston MA Resume Adhar MannaAdharMannaNo ratings yet
- Motivated Skepticism in The Evaluation of Political BeliefsDocument16 pagesMotivated Skepticism in The Evaluation of Political BeliefsAnonymous I56qtCNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Eng4. ElementsDocument8 pagesEng4. Elementsmierene cabilloNo ratings yet
- MOEd Secondary SchoolsDocument1 pageMOEd Secondary SchoolsSAR Official AudioNo ratings yet
- DissertationDocument118 pagesDissertationNatalia Canales CanalesNo ratings yet
- Public Storm Warning Signal (PSWS)Document5 pagesPublic Storm Warning Signal (PSWS)Jeric Rey AuditorNo ratings yet
- Articles Training GuideDocument156 pagesArticles Training GuidescribdgiridarNo ratings yet
- The Abington Journal 02-01-2012Document20 pagesThe Abington Journal 02-01-2012The Times LeaderNo ratings yet
- Air-in-Line Alarms: Decreasing Alarms Through Antisiphon Valve ImplementationDocument3 pagesAir-in-Line Alarms: Decreasing Alarms Through Antisiphon Valve ImplementationSjis11362No ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Competence-Based Learning Materials: Sector: TourismDocument68 pagesCompetence-Based Learning Materials: Sector: TourismAnalizaViloriaNo ratings yet
- Monthly Meeting English - Filipino Club: TH RDDocument3 pagesMonthly Meeting English - Filipino Club: TH RDMerben AlmioNo ratings yet
- Project Management CapstoneDocument251 pagesProject Management CapstoneDSunte WilsonNo ratings yet
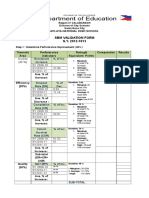
- SBM VAlidation FormDocument2 pagesSBM VAlidation FormamerizaNo ratings yet
- Vocabulary Standard Unit 09Document2 pagesVocabulary Standard Unit 09irenesglez9No ratings yet
- Polytechnic LecturerDocument4 pagesPolytechnic LecturersambhudharmadevanNo ratings yet
- Unit Outline: School of Biomedical Biomolecular and Chemical SciencesDocument4 pagesUnit Outline: School of Biomedical Biomolecular and Chemical SciencesEvilasio CostaNo ratings yet
- Love Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)From EverandLove Life: How to Raise Your Standards, Find Your Person, and Live Happily (No Matter What)Rating: 3 out of 5 stars3/5 (1)