You might also like
- 6 - AnamnesisDocument7 pages6 - Anamnesislouie john abilaNo ratings yet
- A Case Report - Mini Mental Status ExaminationDocument6 pagesA Case Report - Mini Mental Status ExaminationShraddha100% (2)
- Aaron Decena's Psychological Report and Treatment PlanDocument4 pagesAaron Decena's Psychological Report and Treatment Plancaparasangelam69% (13)
- Timeline of Historical Events in Clinical Psychology in The PhilippinesDocument7 pagesTimeline of Historical Events in Clinical Psychology in The PhilippinesAlexandra100% (2)
- Psychological Report of SR - DeseoDocument3 pagesPsychological Report of SR - DeseoRommel SarjNo ratings yet
- Psychia AnamnesisDocument9 pagesPsychia AnamnesisKen Harry MirafuentesNo ratings yet
- Informed Consent To Participate in Psychological Assessment and EvaluationDocument4 pagesInformed Consent To Participate in Psychological Assessment and EvaluationJeffrey CardonaNo ratings yet
- Psych Assessment 1Document13 pagesPsych Assessment 1Ronald Jacob PicorroNo ratings yet
- Depression Case StudyDocument9 pagesDepression Case StudySara Lynn LeSage86% (7)
- PSYCHreportDocument4 pagesPSYCHreportjoyce ramirezNo ratings yet
- Case Study of Ptsd..Document3 pagesCase Study of Ptsd..Crislyn DaepNo ratings yet
- Rehabilitation Center Psychological ReportDocument8 pagesRehabilitation Center Psychological Reportadrian08No ratings yet
- Complete Guide to the Mental Status ExaminationDocument6 pagesComplete Guide to the Mental Status ExaminationnickyboreNo ratings yet
- Psychological Assessment: (Insert and PDF Palihug Te Hehe)Document6 pagesPsychological Assessment: (Insert and PDF Palihug Te Hehe)Casas, Jo-an Pauline A.100% (1)
- Generalized Anxiety Disorder A Case Study Submitted byDocument24 pagesGeneralized Anxiety Disorder A Case Study Submitted bySHARMAINE ANNE POLICIOS0% (1)
- PSYCH REPORT (Sample)Document11 pagesPSYCH REPORT (Sample)mspsy89% (18)
- SSCT Sample Report 1Document1 pageSSCT Sample Report 1Nazema_Sagi40% (5)
- Case Report of PatientDocument25 pagesCase Report of PatientMaria Qibtia100% (2)
- Case Study of Bipolar DisorderDocument1 pageCase Study of Bipolar DisorderIrene Mae Villanueva Ariola0% (1)
- Psychiatric Case StudyDocument12 pagesPsychiatric Case Studyapi-353526506100% (1)
- Psychological Report Mental Health AssessmentDocument4 pagesPsychological Report Mental Health AssessmentRochelle Joyce Olmilla Bersamin67% (3)
- Anamnesis FinaleDocument13 pagesAnamnesis FinaleCaracel Cabrera SobionoNo ratings yet
- Psychological Report Unedited (BN)Document4 pagesPsychological Report Unedited (BN)Aerin50% (4)
- Reasons for referral, assessment procedures, background, observations, test results, interpretations in psychological reportsDocument4 pagesReasons for referral, assessment procedures, background, observations, test results, interpretations in psychological reportsCarla JoyceNo ratings yet
- Undifferentiated Schizophrenia Case Study SampleDocument202 pagesUndifferentiated Schizophrenia Case Study SampleSaro Balberan86% (7)
- Psych Report - SSCTDocument5 pagesPsych Report - SSCTLiza Obtial BrionesNo ratings yet
- Sample Psychological ReportDocument11 pagesSample Psychological ReportFrancisDrona80% (5)
- Case History ReportDocument27 pagesCase History Reportdivya100% (2)
- Sample Psychological Report - ConfidentialDocument19 pagesSample Psychological Report - ConfidentialCeline Sto Domingo - Enriquez68% (22)
- Neuropsychological report reveals trauma symptomsDocument10 pagesNeuropsychological report reveals trauma symptomsadrian Yrigan100% (1)
- Reflection PaperDocument2 pagesReflection PaperVia RoderosNo ratings yet
- Case Study - Binge Eating DisorderDocument5 pagesCase Study - Binge Eating Disorderapi-4264283210% (1)
- Basic Personality Inventory (Bpi)Document14 pagesBasic Personality Inventory (Bpi)Roxanne Forbes100% (1)
- Anamnesis SampleDocument7 pagesAnamnesis SampleKaloy Kamao100% (2)
- Case 1 SchizophreniaDocument4 pagesCase 1 Schizophreniabent78100% (1)
- Anxiety NeurosisDocument34 pagesAnxiety Neurosisilakkiya ilakkiyaNo ratings yet
- Case Study PTSD FinalDocument4 pagesCase Study PTSD Finalapi-242142838No ratings yet
- MENTAL STATUS EXAM ORIENTATIONDocument4 pagesMENTAL STATUS EXAM ORIENTATIONavigaeljoieNo ratings yet
- Psychology Report M.A Report ClinicalDocument15 pagesPsychology Report M.A Report Clinicalterezki67% (3)
- Psychological Report Ni Roy FinalDocument9 pagesPsychological Report Ni Roy Finalrlinao100% (1)
- Catatonic Schizophrenia SymptomsDocument13 pagesCatatonic Schizophrenia SymptomsWen Silver100% (1)
- RGO Psychological Assessment Enhanced 2016 1Document335 pagesRGO Psychological Assessment Enhanced 2016 1Esther Faith Montilla100% (1)
- OCD Case StudyDocument14 pagesOCD Case Studyvidushi yadav100% (1)
- Mental Status ExamDocument8 pagesMental Status ExamKhaled GharaibehNo ratings yet
- Psychopathology of SchizophreniaDocument2 pagesPsychopathology of SchizophreniaJhe MallariNo ratings yet
- Psychological Report FormatDocument3 pagesPsychological Report FormatAn Jannette AlmodielNo ratings yet
- Assessment Profile ReportDocument1 pageAssessment Profile ReportChai Aries50% (4)
- Bipolar 1 Case PresentationDocument111 pagesBipolar 1 Case PresentationJhensczy Hazel Maye AlbaNo ratings yet
- Psychiatry Case Report TemplateDocument3 pagesPsychiatry Case Report TemplateMuhamad Aizat75% (4)
- OJT Report at NCMH Mental Health CenterDocument25 pagesOJT Report at NCMH Mental Health Centerpaul william lalataNo ratings yet
- Schizophrenia Case StudyDocument24 pagesSchizophrenia Case StudyRichard Sy100% (3)
- Psychological Assessment Chapter 10Document2 pagesPsychological Assessment Chapter 10Angel Sta. MariaNo ratings yet
- Psychiatric Case PresentationDocument73 pagesPsychiatric Case PresentationRechie Gallo50% (2)
- Ab Psych Review Lecture Boards With Answers 05.15Document12 pagesAb Psych Review Lecture Boards With Answers 05.15SteffiNo ratings yet
- Meynard Aguilar - PND - Reflection EssayDocument1 pageMeynard Aguilar - PND - Reflection EssayMeynard AguilarNo ratings yet
- History Taking of a 17-Year-Old Male with Addiction and Sexual DysfunctionDocument3 pagesHistory Taking of a 17-Year-Old Male with Addiction and Sexual Dysfunctionmybuddies15875% (12)
- NCMH RequirementsDocument13 pagesNCMH RequirementsRoxanne AquinoNo ratings yet
- Ward Work 1Document6 pagesWard Work 1Jermaine SerranoNo ratings yet
- Case Study CholecystitisDocument33 pagesCase Study CholecystitisMelai de GuzmanNo ratings yet
- Republic of The Philippines Department of Health Baguio General Hospital and Medical Center Psychiatry Department Baguio CityDocument3 pagesRepublic of The Philippines Department of Health Baguio General Hospital and Medical Center Psychiatry Department Baguio CityGerarld Immanuel KairupanNo ratings yet
- Angular Cheilitis - Causes, Symptoms, Treatment and MoreDocument7 pagesAngular Cheilitis - Causes, Symptoms, Treatment and Moremefav7778520No ratings yet
- US Hypertension Review GuidelinesDocument12 pagesUS Hypertension Review Guidelinesmefav7778520100% (1)
- Purine Foods ContentDocument1 pagePurine Foods Contentmefav7778520No ratings yet
- Clinical Clues With Urogenital SyndromeDocument3 pagesClinical Clues With Urogenital Syndromemefav7778520No ratings yet
- Urethritis Testing and TX GuidelinesDocument2 pagesUrethritis Testing and TX Guidelinesmefav7778520No ratings yet
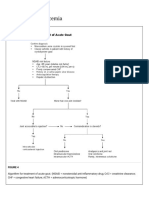
- Algorithm of Acute GoutDocument2 pagesAlgorithm of Acute Goutmefav7778520No ratings yet
- Autism's Top 14 Areas of ConcernDocument2 pagesAutism's Top 14 Areas of Concernmefav7778520No ratings yet
- Bell's Palsy - Differential Diagnosis of Facial Nerve PalsyDocument2 pagesBell's Palsy - Differential Diagnosis of Facial Nerve Palsymefav7778520No ratings yet
- Bell's Palsy - Anatomy of Facial NerveDocument1 pageBell's Palsy - Anatomy of Facial Nervemefav7778520No ratings yet
- Instituting CHANGE in The WorkplaceDocument39 pagesInstituting CHANGE in The Workplacemefav7778520No ratings yet
- Bell's Palsy - Facial Nerve and Supranuclear LesionDocument1 pageBell's Palsy - Facial Nerve and Supranuclear Lesionmefav7778520No ratings yet
- Bell's Palsy: Diagnosis and ManagementDocument2 pagesBell's Palsy: Diagnosis and Managementmefav7778520No ratings yet
- Wms GINA 2017 Main Report Tracked Changes For Archive PDFDocument156 pagesWms GINA 2017 Main Report Tracked Changes For Archive PDFAnnisa MiendaNo ratings yet
- Acute Gout ManagementDocument2 pagesAcute Gout Managementmefav7778520No ratings yet
- ER MEDS LIST WITH COMMON DRUGSDocument3 pagesER MEDS LIST WITH COMMON DRUGSmefav7778520No ratings yet
- UTI Guideline Example 2 Appendix B PDFDocument4 pagesUTI Guideline Example 2 Appendix B PDFamira catriNo ratings yet
- TB in The WorkplaceDocument60 pagesTB in The Workplacemefav7778520100% (1)
- Accident InvestigationDocument39 pagesAccident Investigationmefav7778520No ratings yet
- Industrial HygieneDocument111 pagesIndustrial Hygienemefav7778520100% (1)
- Drug Free WorkplaceDocument91 pagesDrug Free Workplacemefav7778520No ratings yet
- Electrical SafetyDocument35 pagesElectrical Safetymefav7778520No ratings yet
- Emergency Preparedness (Zap)Document24 pagesEmergency Preparedness (Zap)adel santosNo ratings yet
- Compensation MedicineDocument46 pagesCompensation Medicinemefav7778520No ratings yet
- Do 53-03Document6 pagesDo 53-03mefav7778520No ratings yet
- Basic Concept On Toxicology PDFDocument40 pagesBasic Concept On Toxicology PDFmefav7778520No ratings yet
- 5S Industrial HousekeepingDocument17 pages5S Industrial Housekeepingmefav7778520No ratings yet
- Comprehensive and Unified Policy PDFDocument180 pagesComprehensive and Unified Policy PDFmefav7778520No ratings yet
- Accident CausationDocument104 pagesAccident Causationmefav7778520No ratings yet
- Ococ Notes PDFDocument5 pagesOcoc Notes PDFmefav7778520No ratings yet
- Topnotch ECG Interpretation For Moonlighters PDFDocument25 pagesTopnotch ECG Interpretation For Moonlighters PDFmefav7778520No ratings yet
- Laminectomy Definition: Spine Surgery to Relieve Pressure on Spinal Cord or NervesDocument9 pagesLaminectomy Definition: Spine Surgery to Relieve Pressure on Spinal Cord or NervesEdmarie AmistadNo ratings yet
- Gavinos ResumeDocument4 pagesGavinos ResumeRI NANo ratings yet
- Dental Caries IndexDocument35 pagesDental Caries Indexdr parveen bathla100% (1)
- Ch09 AnaestheticsDocument21 pagesCh09 AnaestheticsDonna MitchellNo ratings yet
- AbijitDocument3 pagesAbijitvimalNo ratings yet
- NBEMS announces DNB/DrNB practical exam datesDocument2 pagesNBEMS announces DNB/DrNB practical exam datesShivaraj S ANo ratings yet
- DNB QUESTION PAPER-Topic Wise (Author DR - Sirisha)Document92 pagesDNB QUESTION PAPER-Topic Wise (Author DR - Sirisha)Sirisha CkvNo ratings yet
- Stomach CancerDocument14 pagesStomach CancerLamy SNo ratings yet
- NCP (Acute Pain, Episiotomy)Document6 pagesNCP (Acute Pain, Episiotomy)Jenny AjocNo ratings yet
- TTTTDocument26 pagesTTTTMoataz TrabehNo ratings yet
- Gen EpidemiologyDocument88 pagesGen EpidemiologyShibu Sebastian100% (1)
- Chapter 4 A1 Poster Example 2Document3 pagesChapter 4 A1 Poster Example 2Krisna PamungkasNo ratings yet
- Emergency Medical Technician CPGs PDFDocument121 pagesEmergency Medical Technician CPGs PDFAnonymous OdW7ev100% (1)
- Social Participation of People With Chronic Wounds - A Systematic ReviewDocument25 pagesSocial Participation of People With Chronic Wounds - A Systematic ReviewcumbredinNo ratings yet
- Post Op InstructionsDocument5 pagesPost Op InstructionsAmar Bhochhibhoya0% (1)
- Using Enzymes to Diagnose and Treat DiseasesDocument30 pagesUsing Enzymes to Diagnose and Treat DiseasesAnubhav sainiNo ratings yet
- 2015 Case Studies in Pain ManagementDocument545 pages2015 Case Studies in Pain ManagementJose Lavoisier moreiraNo ratings yet
- Nursing Care Plan#2kidneyDocument3 pagesNursing Care Plan#2kidneythubtendrolmaNo ratings yet
- Erectile DysfunctionDocument31 pagesErectile Dysfunctionrahuldtc100% (1)
- Isicem 2021Document90 pagesIsicem 2021labbeneNo ratings yet
- PVC Unido ConDuplicadosDocument1,181 pagesPVC Unido ConDuplicadosJorge Chachaima MarNo ratings yet
- Nursing Care for High-Risk Pregnant MothersDocument40 pagesNursing Care for High-Risk Pregnant MothersAllyza EspirituNo ratings yet
- Upload CM69Document8 pagesUpload CM69christian makaryNo ratings yet
- Biosensors 12 00985 v2Document30 pagesBiosensors 12 00985 v2aqsa javedNo ratings yet
- Article. Neoadjuvant Treatment Response As An Early Response Indicator For Patients With Rectal CancerDocument7 pagesArticle. Neoadjuvant Treatment Response As An Early Response Indicator For Patients With Rectal CancerTrí Cương NguyễnNo ratings yet
- Jurnal Kesehatan Gigi: Perilaku Dan Keterampilan Menyikat Gigi Terhadap Timbulnya Karies Gigi Pada Anak Di Kota JambiDocument7 pagesJurnal Kesehatan Gigi: Perilaku Dan Keterampilan Menyikat Gigi Terhadap Timbulnya Karies Gigi Pada Anak Di Kota JambiUntuk TugasNo ratings yet
- NURSING PRACTICE Test COMMUNITY HEALTH NURSING AND CARE OF THE MOTHER AND CHILDDocument8 pagesNURSING PRACTICE Test COMMUNITY HEALTH NURSING AND CARE OF THE MOTHER AND CHILDJhannNo ratings yet
- Antibodies To Sars-Cov-2 Are Associated With Protection Against ReinfectionDocument30 pagesAntibodies To Sars-Cov-2 Are Associated With Protection Against ReinfectionJimmy A. Camones ObregonNo ratings yet
- The Microbial World & You: NomenclatureDocument9 pagesThe Microbial World & You: NomenclatureApryll DarlineNo ratings yet
- Ludwig's AnginaDocument22 pagesLudwig's AnginaDevavrat SinghNo ratings yet