You might also like
- Sterling Test Prep AP Psychology: Complete Content Review for AP Psychology ExamFrom EverandSterling Test Prep AP Psychology: Complete Content Review for AP Psychology ExamNo ratings yet
- Department of Education: Medical Certificate AbnormalitiesDocument1 pageDepartment of Education: Medical Certificate AbnormalitiesMike PerezNo ratings yet
- Geriatric Case KitDocument6 pagesGeriatric Case KitMay Chelle ErazoNo ratings yet
- Medical Certificate of Athlete: To Whom It May ConcernDocument3 pagesMedical Certificate of Athlete: To Whom It May ConcernRoderick CruzNo ratings yet
- 2020 MedicalCertificate (Combative)Document1 page2020 MedicalCertificate (Combative)Dennmark IgutNo ratings yet
- Pe 2 LKDocument5 pagesPe 2 LKSammy AndyNo ratings yet
- MedicalCertificate For Combative1Document1 pageMedicalCertificate For Combative1Joshua Ponce ToñacaoNo ratings yet
- 2020 MedicalCertificateCombativeDocument1 page2020 MedicalCertificateCombativejefferson pabloNo ratings yet
- 2017 MedicalCertificate For Boxing 1Document1 page2017 MedicalCertificate For Boxing 1JAMES AGUILARNo ratings yet
- MedicalCertificate For Boxing 1 PDFDocument1 pageMedicalCertificate For Boxing 1 PDFKleng ReyesNo ratings yet
- Immersion Medical CertificateDocument1 pageImmersion Medical Certificatejestoni manipolNo ratings yet
- Physicalexam Score SheetDocument2 pagesPhysicalexam Score SheetMarieCrisNo ratings yet
- Prelim Exam Hope 2 I. Choose The Correct Answer From The Box - Right in On The Space ProvidedDocument2 pagesPrelim Exam Hope 2 I. Choose The Correct Answer From The Box - Right in On The Space ProvidedCync KlayNo ratings yet
- Hso G Medical Examination FormDocument1 pageHso G Medical Examination FormorionsrulerNo ratings yet
- Professional Qualities / Patient Care NameDocument1 pageProfessional Qualities / Patient Care Namedgina8800No ratings yet
- St. Paul University Philippines: Training Needs Assessment ToolDocument2 pagesSt. Paul University Philippines: Training Needs Assessment ToolJosette Mae AtanacioNo ratings yet
- 7.1 - MedicalCertificate For Boxing 1Document1 page7.1 - MedicalCertificate For Boxing 1AlemapSueNo ratings yet
- S Satisfactory, US Unsatisfactory, ND Not Done: Slu Clinical Skills Assessment Physical Examination ChecklistDocument3 pagesS Satisfactory, US Unsatisfactory, ND Not Done: Slu Clinical Skills Assessment Physical Examination ChecklistJeffrey RamosNo ratings yet
- Care: Nursing Students' Perspective". Please Do Not Leave Anything UnansweredDocument2 pagesCare: Nursing Students' Perspective". Please Do Not Leave Anything UnansweredTania NovizaNo ratings yet
- Medical Certificate 2010 PalaroDocument4 pagesMedical Certificate 2010 Palarogeard27No ratings yet
- Physical FormDocument2 pagesPhysical Formapi-670925736No ratings yet
- Norsu Health Declaration Form 1 September 2022Document1 pageNorsu Health Declaration Form 1 September 2022Joshua Allen AjetoNo ratings yet
- Migrant Health FormDocument5 pagesMigrant Health FormImelda Junaedi100% (3)
- DPH Form 3300 PDFDocument2 pagesDPH Form 3300 PDFtomtranNo ratings yet
- Foot AssessmentDocument2 pagesFoot AssessmentPalwasha MalikNo ratings yet
- Medical Examination FormDocument1 pageMedical Examination FormShiela A. JalmaniNo ratings yet
- Oral Health Related Quality of Life Following Non Surgical (Routine) Tooth Extraction: A Pilot StudyDocument6 pagesOral Health Related Quality of Life Following Non Surgical (Routine) Tooth Extraction: A Pilot StudyFelipe RoncerosNo ratings yet
- General Form 86Document2 pagesGeneral Form 86Peter a. BoteaNo ratings yet
- Assessing The NailsDocument1 pageAssessing The NailsYousuf Azhar AlamiaNo ratings yet
- Department of Education: First Quarter Mapeh 8 Week2 - Quarter 1Document14 pagesDepartment of Education: First Quarter Mapeh 8 Week2 - Quarter 1Bonifacio LeddaNo ratings yet
- Assessment NailsDocument1 pageAssessment NailsSyphar IndasanNo ratings yet
- MedicalCertificate For Boxing 1Document1 pageMedicalCertificate For Boxing 1Jessie Montes JrNo ratings yet
- Learners Record BookDocument11 pagesLearners Record BookMarjhun Flores GuingayanNo ratings yet
- (HSO) Medical Examination FormDocument1 page(HSO) Medical Examination FormKrizel LagundiNo ratings yet
- Medical For Athletes 1Document3 pagesMedical For Athletes 1Muhammad AlqhaeedNo ratings yet
- Philippine Pediatric Society, INC. Committee On Research Forums and Workshop (FORM CR-100)Document3 pagesPhilippine Pediatric Society, INC. Committee On Research Forums and Workshop (FORM CR-100)OsMak PediatricsNo ratings yet
- Questionnaire ResearchDocument2 pagesQuestionnaire ResearchSHINE JONERY LEBECONo ratings yet
- Department of Education: What's inDocument12 pagesDepartment of Education: What's inBonifacio LeddaNo ratings yet
- Final Veterinarian Statement NecropsyDocument1 pageFinal Veterinarian Statement Necropsyani ni musNo ratings yet
- Francais sport-WORKSHEETDocument1 pageFrancais sport-WORKSHEETrite2shinjiniNo ratings yet
- 2017MedicalCertificate For Combative 1Document2 pages2017MedicalCertificate For Combative 1Aloha Aguilar BrusasNo ratings yet
- Medical Certificate: (Arnis, Boxing, Taekwondo, Gymnastics, Wrestling & Wushu)Document2 pagesMedical Certificate: (Arnis, Boxing, Taekwondo, Gymnastics, Wrestling & Wushu)Aloha Aguilar BrusasNo ratings yet
- 2017 MedicalCertificate For Boxing 2Document1 page2017 MedicalCertificate For Boxing 2Angelou GalonNo ratings yet
- Medical FormDocument2 pagesMedical FormDuván ArleyNo ratings yet
- Quiz ShsDocument3 pagesQuiz ShsJonel LicupNo ratings yet
- Patient TraumaDocument1 pagePatient Traumacptjimmy15No ratings yet
- Medical Form.Document4 pagesMedical Form.victoremai76No ratings yet
- Medical CertificateDocument1 pageMedical CertificateNarito ArnelNo ratings yet
- Medical Certificate23Document1 pageMedical Certificate23Donna Karen MoronNo ratings yet
- Physical Activity Readiness Questionnaire (Par Q) : Regional Medical and Dental Unit 7Document2 pagesPhysical Activity Readiness Questionnaire (Par Q) : Regional Medical and Dental Unit 7Kate YuragNo ratings yet
- Physical Examination Certificate: (To Be Completed by Medical Doctor)Document2 pagesPhysical Examination Certificate: (To Be Completed by Medical Doctor)Brain Sharpeners - KoreanNo ratings yet
- Medical Pro Form ADocument5 pagesMedical Pro Form Atanujchopra1No ratings yet
- Speech Pathology Preceptor - Name Title Initials Boston Medical CenterDocument2 pagesSpeech Pathology Preceptor - Name Title Initials Boston Medical CenterleslieNo ratings yet
- Health 7 1st Quiz #02 Health Concerns and Health AppraisalDocument2 pagesHealth 7 1st Quiz #02 Health Concerns and Health Appraisalryan bersaminNo ratings yet
- Medical Certificate: To Whom It May ConcernDocument1 pageMedical Certificate: To Whom It May ConcernDexter Emnas AbergonzadoNo ratings yet
- Surgery/Anesthesia Release FormDocument1 pageSurgery/Anesthesia Release FormArchetype ProductionsNo ratings yet
- Patient Assessment Form: Assess Scene Secondary SurveyDocument2 pagesPatient Assessment Form: Assess Scene Secondary Surveydeepeezee_beenNo ratings yet
- Dental Examination Record FormDocument1 pageDental Examination Record FormDave Love NemialyNo ratings yet
- 2017 MedicalCertificate For Boxing 2Document1 page2017 MedicalCertificate For Boxing 2Majhi PeraltaNo ratings yet
- PDS CCM Lic PracDocument6 pagesPDS CCM Lic PracmachesoNo ratings yet
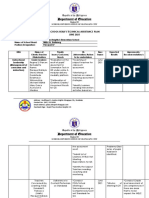
- Department of Education: School Head'S Technical Assistance Plan JUNE 2021Document7 pagesDepartment of Education: School Head'S Technical Assistance Plan JUNE 2021Annabelle Poniente HertezNo ratings yet
- Reporter: Nove Joy L. Deleña Bsed-Bio - Sci. IiiDocument7 pagesReporter: Nove Joy L. Deleña Bsed-Bio - Sci. IiiAnnabelle Poniente HertezNo ratings yet
- Department of Education: School Head'S Technical Assistance Reporting Log APRIL 2021Document18 pagesDepartment of Education: School Head'S Technical Assistance Reporting Log APRIL 2021Annabelle Poniente HertezNo ratings yet
- Department of Education: School Head'S Technical Assistance Plan MAY 2021Document8 pagesDepartment of Education: School Head'S Technical Assistance Plan MAY 2021Annabelle Poniente HertezNo ratings yet
- The Use of Organic FertilizerDocument15 pagesThe Use of Organic FertilizerAnnabelle Poniente HertezNo ratings yet
- Template Business PlanDocument5 pagesTemplate Business PlanAnnabelle Poniente HertezNo ratings yet
- Department of Education: Monthly Supervisory Accomplishment Report November 2020Document4 pagesDepartment of Education: Monthly Supervisory Accomplishment Report November 2020Annabelle Poniente HertezNo ratings yet
- Las Science4 q2w2Document2 pagesLas Science4 q2w2Annabelle Poniente HertezNo ratings yet
- Principle of AssessmentDocument43 pagesPrinciple of AssessmentAnnabelle Poniente HertezNo ratings yet
- PFR Assignment Parental AuthorityDocument14 pagesPFR Assignment Parental AuthorityAnnabelle Poniente HertezNo ratings yet
- BSP Plastic Container PlantersDocument5 pagesBSP Plastic Container PlantersAnnabelle Poniente HertezNo ratings yet
- Cookies (100pcs) Quantity Price/Quantity Total AmountDocument3 pagesCookies (100pcs) Quantity Price/Quantity Total AmountAnnabelle Poniente HertezNo ratings yet
- Business Plan DETAILDocument4 pagesBusiness Plan DETAILAnnabelle Poniente HertezNo ratings yet
- Effects of The Environment On The Life Cycle of Organisms: Worksheet in Science IvDocument2 pagesEffects of The Environment On The Life Cycle of Organisms: Worksheet in Science IvAnnabelle Poniente Hertez100% (1)
- Stages in The Life Cycle of Organisms: Worksheet in Science IvDocument2 pagesStages in The Life Cycle of Organisms: Worksheet in Science IvAnnabelle Poniente Hertez0% (1)
- Body Structures That Help Animals Adapt and Survive: Worksheet in Science IvDocument2 pagesBody Structures That Help Animals Adapt and Survive: Worksheet in Science IvAnnabelle Poniente HertezNo ratings yet
- Ghies Teachers Study Notebook LDM Module Course 2Document45 pagesGhies Teachers Study Notebook LDM Module Course 2Annabelle Poniente Hertez100% (1)
- ERF CertificationDocument1 pageERF CertificationAnnabelle Poniente HertezNo ratings yet
- Cav FormsDocument17 pagesCav FormsAnnabelle Poniente HertezNo ratings yet
- Sworn Statement ERFDocument4 pagesSworn Statement ERFAnnabelle Poniente Hertez100% (1)
- Support HandbookDocument68 pagesSupport HandbookAnnabelle Poniente Hertez100% (1)
- Commitment: Republic of The Philippines Department of Education Region III Olongapo CityDocument1 pageCommitment: Republic of The Philippines Department of Education Region III Olongapo CityAnnabelle Poniente HertezNo ratings yet
- Check DisbursementDocument16 pagesCheck DisbursementAnnabelle Poniente HertezNo ratings yet
- Request For Quotation: Gordon Heights I Elementary SchoolDocument1 pageRequest For Quotation: Gordon Heights I Elementary SchoolAnnabelle Poniente HertezNo ratings yet
- Lecture On Lis Bosy 2016 For Adviser Account by Alfredo Medrano 2Document30 pagesLecture On Lis Bosy 2016 For Adviser Account by Alfredo Medrano 2Annabelle Poniente HertezNo ratings yet
- Effective Classroom Management TechniquesDocument53 pagesEffective Classroom Management TechniquesAnnabelle Poniente Hertez100% (2)
- For Grade V Pupils For School Year 2017-2018: Use of Technology To Make Science Classroom More Engaging and RelevantDocument11 pagesFor Grade V Pupils For School Year 2017-2018: Use of Technology To Make Science Classroom More Engaging and RelevantAnnabelle Poniente HertezNo ratings yet