You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Alveolar bone formation and structureDocument16 pagesAlveolar bone formation and structuremirfanulhaqNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Pros QuestionsDocument7 pagesPros QuestionsmirfanulhaqNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Peds Restorative PDFDocument4 pagesPeds Restorative PDFmirfanulhaqNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Management of Cracked TeethDocument6 pagesManagement of Cracked Teethsaifuddin suhri100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Gingival InflammationDocument19 pagesGingival InflammationmirfanulhaqNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Pulp Protection Methods and MaterialsDocument13 pagesPulp Protection Methods and MaterialsmirfanulhaqNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Pros Exam 1 2003Document8 pagesPros Exam 1 2003mirfanulhaqNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Pros Exam 1 2002Document8 pagesPros Exam 1 2002mirfanulhaqNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Comprehensive Periodontal Exam GuideDocument40 pagesComprehensive Periodontal Exam GuideKavin SandhuNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Pros Exam 1 2002Document8 pagesPros Exam 1 2002mirfanulhaqNo ratings yet
- Oral InfectionsDocument14 pagesOral InfectionsmirfanulhaqNo ratings yet
- Anticoagulation GuidelinesDocument2 pagesAnticoagulation GuidelinesmirfanulhaqNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Complications in Dentoalveolar Surgery PDFDocument37 pagesComplications in Dentoalveolar Surgery PDFmirfanulhaqNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Wound Healing PDFDocument7 pagesWound Healing PDFmirfanulhaqNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Adhesion SystemsDocument13 pagesAdhesion SystemsTolean AndreeviciNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Fundamentals of SalivaDocument15 pagesFundamentals of SalivasreedamNo ratings yet
- Pulp 2008 HandoutDocument7 pagesPulp 2008 HandoutNemanja MiticNo ratings yet
- 2 Saliva PhysiologyDocument20 pages2 Saliva PhysiologyvelangniNo ratings yet
- Guide to Fluoride TherapyDocument4 pagesGuide to Fluoride TherapymirfanulhaqNo ratings yet
- Pulp Protection Methods and MaterialsDocument13 pagesPulp Protection Methods and MaterialsmirfanulhaqNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Making Sense of Mouth Ulceration 5Document3 pagesMaking Sense of Mouth Ulceration 5mirfanulhaqNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Oral Healthcare Considerations For The Pregnant WomanDocument4 pagesOral Healthcare Considerations For The Pregnant WomanmirfanulhaqNo ratings yet
- Scully Oral UlcersDocument3 pagesScully Oral UlcersdeenmNo ratings yet
- Making Sense of Mouth Ulceration 6Document3 pagesMaking Sense of Mouth Ulceration 6mirfanulhaqNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Making Sense of Mouth Ulceration 3Document4 pagesMaking Sense of Mouth Ulceration 3mirfanulhaqNo ratings yet
- Opath - Most Common ListDocument4 pagesOpath - Most Common ListmirfanulhaqNo ratings yet
- Making Sense of Mouth Ulceration 6Document3 pagesMaking Sense of Mouth Ulceration 6mirfanulhaqNo ratings yet
- Scully Oral UlcersDocument3 pagesScully Oral UlcersdeenmNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Scully Oral UlcersDocument3 pagesScully Oral UlcersdeenmNo ratings yet
- Risk factors for MDR-TB in DG Khan & MuzaffargarhDocument12 pagesRisk factors for MDR-TB in DG Khan & MuzaffargarhDr.Abuzar ShiraniNo ratings yet
- Recognizing Interstitial Versus Airspace Disease Recognizing Interstitial Versus Airspace DiseaseDocument30 pagesRecognizing Interstitial Versus Airspace Disease Recognizing Interstitial Versus Airspace DiseaseYoga KharismaNo ratings yet
- Pneumonia lobara la copilDocument115 pagesPneumonia lobara la copilIonut Horgot100% (2)
- 4973618841167dcf734ab5fa9d6c6f47Document8 pages4973618841167dcf734ab5fa9d6c6f47Nazarii KordupelNo ratings yet
- LAPORAN INDIVIDU TUBERKULOSIS PARUDocument44 pagesLAPORAN INDIVIDU TUBERKULOSIS PARURahmawati AzmiNo ratings yet
- Modul-2 Pengobatan TBDocument180 pagesModul-2 Pengobatan TBJane BiringanNo ratings yet
- TUBERCULOSISDocument25 pagesTUBERCULOSISManuel Fatima Goncalves83% (6)
- 8 DotsDocument44 pages8 DotsjyuldipNo ratings yet
- Jasmin 1Document22 pagesJasmin 1angel angelNo ratings yet
- SandozDocument22 pagesSandozDewa SuryaNo ratings yet
- Childhood TB MCQ QuizDocument21 pagesChildhood TB MCQ QuizSaya Menang75% (4)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- MTB TITLEDocument30 pagesMTB TITLEFanny BudimanNo ratings yet
- Gambaran Karakteristik Pneumonia Pada Anak Yang Dirawat Di Ruang Perawatan Intensif Anak RSUP Prof. Dr. R. D. Kandou Manado Periode 2013 - 2015Document9 pagesGambaran Karakteristik Pneumonia Pada Anak Yang Dirawat Di Ruang Perawatan Intensif Anak RSUP Prof. Dr. R. D. Kandou Manado Periode 2013 - 2015Tedi NovanNo ratings yet
- Presentation Outline Nursing Pulmonary Tuberculosis Revised 1Document10 pagesPresentation Outline Nursing Pulmonary Tuberculosis Revised 1Alfaera Rahma FarestyNo ratings yet
- Pengaruh Perilaku Dan Status Gizi Terhadap Kejadian TB Paru Di Kota PekalonganDocument40 pagesPengaruh Perilaku Dan Status Gizi Terhadap Kejadian TB Paru Di Kota PekalonganAnonymous PGuZwT0IKNo ratings yet
- Biology Project On TBDocument20 pagesBiology Project On TBAdnan Fazeel73% (15)
- TB ReportDocument33 pagesTB ReportAAZEEN ALINo ratings yet
- gtbr14 Main Text PDFDocument134 pagesgtbr14 Main Text PDFAnonymous fqa7PO8oNo ratings yet
- Tuberculosis: Dr. Shami Pokhrel Dept. of Pediatrics, LMCDocument37 pagesTuberculosis: Dr. Shami Pokhrel Dept. of Pediatrics, LMCShami PokhrelNo ratings yet
- TB CPG Map by DR Syafiq SalhadiDocument1 pageTB CPG Map by DR Syafiq SalhadirebeccaNo ratings yet
- Rifampin ResistanceDocument4 pagesRifampin ResistanceHeldrian dwinanda SuyuthieNo ratings yet
- A Thesis: Assessment of Prevalence of All Form of TB Cases in Bedessa Health Center West Harerge, Oromia Region, EthiopiaDocument29 pagesA Thesis: Assessment of Prevalence of All Form of TB Cases in Bedessa Health Center West Harerge, Oromia Region, EthiopiaFisehaNo ratings yet
- PCV Septia 2003Document16 pagesPCV Septia 2003WondaNo ratings yet
- Multiple Choice Questions: Mycobacterium TuberculosisDocument31 pagesMultiple Choice Questions: Mycobacterium Tuberculosisdoan luong100% (6)
- Daftar PustakaDocument8 pagesDaftar PustakaRachel VictorianaNo ratings yet
- Grania Brigden's Webinar Presentation - Scientific Highlights of 47th Union World Conf On Lung Health in LiverpoolDocument9 pagesGrania Brigden's Webinar Presentation - Scientific Highlights of 47th Union World Conf On Lung Health in LiverpoolbobbyramakantNo ratings yet
- Two Step TSTDocument2 pagesTwo Step TSTBrianHoNo ratings yet
- Saida, Syamsiar : Volume 7 Nomor 1 Bulan Oktober 2019 EISSN: 2443-0218Document9 pagesSaida, Syamsiar : Volume 7 Nomor 1 Bulan Oktober 2019 EISSN: 2443-0218neno fitriyani hasbieNo ratings yet
- (2020) Treatment Outcome of Tuberculosis Treatment Regimens in Kandahar, AfghanistanDocument7 pages(2020) Treatment Outcome of Tuberculosis Treatment Regimens in Kandahar, AfghanistanBilal Ahmad RahimiNo ratings yet
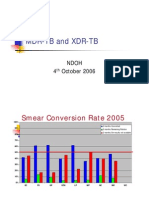
- MDR-TB and XDR-TB: Ndoh 4 October 2006Document40 pagesMDR-TB and XDR-TB: Ndoh 4 October 2006Eta Calvin ObenNo ratings yet
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionFrom EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionRating: 4 out of 5 stars4/5 (402)
- Why We Die: The New Science of Aging and the Quest for ImmortalityFrom EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityRating: 3.5 out of 5 stars3.5/5 (2)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisFrom EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisRating: 4 out of 5 stars4/5 (1)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedFrom EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedRating: 5 out of 5 stars5/5 (78)
- The Age of Magical Overthinking: Notes on Modern IrrationalityFrom EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityRating: 4 out of 5 stars4/5 (13)