You might also like
- The Palliative Approach: A Resource for Healthcare WorkersFrom EverandThe Palliative Approach: A Resource for Healthcare WorkersRating: 4.5 out of 5 stars4.5/5 (3)
- Palliative CareDocument23 pagesPalliative CareCharles Frank100% (1)
- Palliative Care in Bangladesh: Group: IDocument38 pagesPalliative Care in Bangladesh: Group: IShipra TalukderNo ratings yet
- 1rika Konsep PaliatifDocument47 pages1rika Konsep PaliatifRahmi Ferdila Comate SoniqNo ratings yet
- Crtitical Care Nursing: Imran Yousafzai BSN, MSPH, PGHRHM, Mhpe Lecturer KMUDocument42 pagesCrtitical Care Nursing: Imran Yousafzai BSN, MSPH, PGHRHM, Mhpe Lecturer KMUikram ullah khanNo ratings yet
- Palliative CareDocument36 pagesPalliative CareAzka Revan0% (1)
- End of Life CareDocument80 pagesEnd of Life CareRakesh MohanNo ratings yet
- Elective I: Hospice Pallative Care: Mrs. Diane Zaraspe Regalado-RN MANDocument330 pagesElective I: Hospice Pallative Care: Mrs. Diane Zaraspe Regalado-RN MANVianne ArcenioNo ratings yet
- Evidence Based Nursing Practice: BY Summaira Nasir Senior LecturerDocument32 pagesEvidence Based Nursing Practice: BY Summaira Nasir Senior LecturerSumera ShaheenNo ratings yet
- The Nurses Role in Palliative Care A QualitativeDocument18 pagesThe Nurses Role in Palliative Care A Qualitativesukarni84sgdNo ratings yet
- RolesDocument13 pagesRolesGeorgeEchevarriaNo ratings yet
- Palliative CareDocument64 pagesPalliative Caremillstoneridge150% (2)
- Introduction To PALLIATIVE CAREDocument73 pagesIntroduction To PALLIATIVE CARERajesh T Eapen100% (1)
- The Role of The Nurse in Palliative Care Settings in A Global ContextDocument6 pagesThe Role of The Nurse in Palliative Care Settings in A Global Context_astyNo ratings yet
- Florence Nightingale-Modern NursingDocument25 pagesFlorence Nightingale-Modern NursingRanah Julia Garchitorena Ayo100% (1)
- DNP Implementation of A Depression Screening Program Among Older Adults in The Primary Care Setting Utilizing The Geriatric Depression ScaleDocument80 pagesDNP Implementation of A Depression Screening Program Among Older Adults in The Primary Care Setting Utilizing The Geriatric Depression ScaleDerin Colvin100% (2)
- The Solid Facts - Palliative Care PDFDocument35 pagesThe Solid Facts - Palliative Care PDFDamarys DecothéNo ratings yet
- Frailty SyndromeDocument24 pagesFrailty SyndromeRinaldyAlexanderNo ratings yet
- Palliative Care: Basic TerminologiesDocument7 pagesPalliative Care: Basic TerminologiesDagmawit GirmaNo ratings yet
- Collaborative Care Between Nurse Practitioners and Primary Care PhysiciansDocument11 pagesCollaborative Care Between Nurse Practitioners and Primary Care PhysiciansLeek AgoessNo ratings yet
- Electroconvulsive Therapy (ECT) PPT OdeDocument4 pagesElectroconvulsive Therapy (ECT) PPT OdeSatya IndraNo ratings yet
- A Syllabus For Fellowship Education in Palliative MedicineDocument12 pagesA Syllabus For Fellowship Education in Palliative Medicinebaixinha_No ratings yet
- Standards of Psychiatric Mental Health NursingDocument33 pagesStandards of Psychiatric Mental Health NursingSANU RAMASWAMY100% (1)
- Crtitical Care Nursing-3Document47 pagesCrtitical Care Nursing-3AamirNo ratings yet
- Psychosocial NursingDocument21 pagesPsychosocial NursingAngeline Angeles100% (1)
- Palliative CareDocument153 pagesPalliative Carerlinao100% (3)
- Palliative CareDocument35 pagesPalliative CareChucky Vergara75% (4)
- Palliative CareDocument8 pagesPalliative Careapi-402433242No ratings yet
- Improving The Quality of Care in An Acute Care Facility Through RDocument88 pagesImproving The Quality of Care in An Acute Care Facility Through RNor-aine Salazar AccoyNo ratings yet
- Palliative Care Nursing - S. Payne, J. Seymour, C. Ingleton (Open Univ. Press, 2004) WW PDFDocument805 pagesPalliative Care Nursing - S. Payne, J. Seymour, C. Ingleton (Open Univ. Press, 2004) WW PDFpouiftfvo100% (3)
- Reflection About Palliative Care and End of Life CareDocument5 pagesReflection About Palliative Care and End of Life CareVILLEJO JHOVIALENNo ratings yet
- Research in Palliative Care PresentationDocument20 pagesResearch in Palliative Care PresentationNICKY SAMBONo ratings yet
- Cardiopulmonary Assessment and InterventionDocument51 pagesCardiopulmonary Assessment and InterventionPreciousShaizNo ratings yet
- The Evolution of Professional NursingDocument32 pagesThe Evolution of Professional NursingNatukunda DianahNo ratings yet
- Psych - Nursing InterventionsDocument23 pagesPsych - Nursing Interventionsmarie100% (19)
- Health Assessment in NursingDocument4 pagesHealth Assessment in NursingKiara Ash BeethovenNo ratings yet
- Psychiatric Mental Health Case StudyDocument11 pagesPsychiatric Mental Health Case Studyapi-402701741100% (1)
- 4140 Philosophy of NursingDocument10 pages4140 Philosophy of Nursingapi-402049640No ratings yet
- Handbook of Geriatric Nursing Care (PDFDrive) PDFDocument676 pagesHandbook of Geriatric Nursing Care (PDFDrive) PDFPotato BananaNo ratings yet
- AppendicitisDocument8 pagesAppendicitisPhoebe Corazon Cercado100% (1)
- Nursing Department: Saint Mary's UniversityDocument6 pagesNursing Department: Saint Mary's UniversityCheetah GemmaNo ratings yet
- Emergency NursingDocument16 pagesEmergency NursingSwapnil Mahapure100% (2)
- Spinal Cord Injury: Mrs. Zaida ZaracenaDocument36 pagesSpinal Cord Injury: Mrs. Zaida ZaracenaArdhel LoslosoNo ratings yet
- Module-1 Introduction To Geriatric DisordersDocument8 pagesModule-1 Introduction To Geriatric DisordersAshani AaroraNo ratings yet
- 130300-Standards For Acute and Critical Care NursingDocument12 pages130300-Standards For Acute and Critical Care Nursingapi-315277523No ratings yet
- Ventilator-Associated Pneumonia - Risk Factors & Prevention (Beth Augustyn)Document8 pagesVentilator-Associated Pneumonia - Risk Factors & Prevention (Beth Augustyn)ariepitonoNo ratings yet
- Palliative Care Tim - Setting - ModelDocument42 pagesPalliative Care Tim - Setting - ModelNur Fattah100% (1)
- Care of The Acutely Unwell FinalDocument100 pagesCare of The Acutely Unwell Finalgireeshsachin100% (1)
- Ethical Issues in AnaesthesiaDocument23 pagesEthical Issues in AnaesthesiaEverton McIntosh0% (1)
- SOP TemplateDocument2 pagesSOP TemplatePaulin NiyomugaboNo ratings yet
- Acute Coronary SyndromeDocument4 pagesAcute Coronary SyndromeHaryaman JustisiaNo ratings yet
- SBAR ToolkitDocument48 pagesSBAR ToolkitRidwan Ari AntoNo ratings yet
- Request Letter For PreceptorshipDocument2 pagesRequest Letter For PreceptorshipRon OpulenciaNo ratings yet
- Critical AppraisalDocument17 pagesCritical Appraisallowella100% (3)
- Introduction To ECG For NursingDocument75 pagesIntroduction To ECG For NursingRashid AlHamdan100% (1)
- Humanism, Nursing, Communication and Holistic Care: a Position Paper: Position PaperFrom EverandHumanism, Nursing, Communication and Holistic Care: a Position Paper: Position PaperNo ratings yet
- Nurses and Their Patients: Informing practice through psychodynamic insightsFrom EverandNurses and Their Patients: Informing practice through psychodynamic insightsNo ratings yet
- Fundamental Aspects of Palliative Care Nursing 2nd Edition: An Evidence-Based Handbook for Student NursesFrom EverandFundamental Aspects of Palliative Care Nursing 2nd Edition: An Evidence-Based Handbook for Student NursesNo ratings yet
- Hospice Palliative Home Care and Bereavement Support: Nursing Interventions and Supportive CareFrom EverandHospice Palliative Home Care and Bereavement Support: Nursing Interventions and Supportive CareLorraine HoltslanderNo ratings yet
- Republic Vs de GraciaDocument5 pagesRepublic Vs de GraciaRuiz Arenas AgacitaNo ratings yet
- Scra 2014Document3 pagesScra 2014Czara DyNo ratings yet
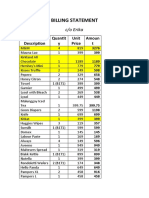
- S&R - Billing StatementDocument4 pagesS&R - Billing StatementCzara DyNo ratings yet
- Republic Vs de GraciaDocument5 pagesRepublic Vs de GraciaRuiz Arenas AgacitaNo ratings yet
- BlaaaaaaaahDocument1 pageBlaaaaaaaahCzara DyNo ratings yet
- Barcelote Vs - RepublicDocument2 pagesBarcelote Vs - RepublicCzara DyNo ratings yet
- Marie Ivonne F. Reyes: Pasig Catholic SchoolDocument1 pageMarie Ivonne F. Reyes: Pasig Catholic SchoolCzara DyNo ratings yet
- Garcia vs. RecioDocument2 pagesGarcia vs. RecioCzara DyNo ratings yet
- Policarpio Vs Active BankDocument2 pagesPolicarpio Vs Active BankCzara DyNo ratings yet
- Lacerna Vs CorcinoDocument2 pagesLacerna Vs CorcinobenNo ratings yet
- CORPPPPPPPOOOOOOOOODocument2 pagesCORPPPPPPPOOOOOOOOOCzara DyNo ratings yet
- Corpo Notes 2018 PrelimsDocument14 pagesCorpo Notes 2018 PrelimsCzara DyNo ratings yet
- Barcelote Vs - RepublicDocument2 pagesBarcelote Vs - RepublicCzara DyNo ratings yet
- Castillo vs. RepublicDocument2 pagesCastillo vs. RepublicCzara DyNo ratings yet
- Corpo PrelimsDocument67 pagesCorpo PrelimsCzara DyNo ratings yet
- Policarpio Vs Active BankDocument2 pagesPolicarpio Vs Active BankCzara DyNo ratings yet
- Fujiki vs. MarinayDocument2 pagesFujiki vs. MarinayCzara DyNo ratings yet
- G.R. No. L-48955, June 30, 1987)Document8 pagesG.R. No. L-48955, June 30, 1987)Czara DyNo ratings yet
- G.R. No. L-48955, June 30, 1987)Document8 pagesG.R. No. L-48955, June 30, 1987)Czara DyNo ratings yet
- Institution of Heirs. It Will Not Result To IntestacyDocument9 pagesInstitution of Heirs. It Will Not Result To IntestacyCzara DyNo ratings yet
- Sunio v. NLRCDocument3 pagesSunio v. NLRCCzara DyNo ratings yet
- Banking Mon 7718Document2 pagesBanking Mon 7718Czara DyNo ratings yet
- Torts Finals Pages 15-19Document3 pagesTorts Finals Pages 15-19Czara DyNo ratings yet
- Proximate or Legal Cause To Legal InjuryDocument12 pagesProximate or Legal Cause To Legal InjuryCzara DyNo ratings yet
- Q&A Wills Dean AligadaDocument5 pagesQ&A Wills Dean AligadaCzara DyNo ratings yet
- Nil Cases FinalsDocument37 pagesNil Cases FinalsCzara DyNo ratings yet
- Page 7 - 8 Proximate or Legal Cause To Legal InjuryDocument12 pagesPage 7 - 8 Proximate or Legal Cause To Legal InjuryCzara DyNo ratings yet
- Evidence PPT 2018 - Dy NotesDocument14 pagesEvidence PPT 2018 - Dy NotesCzara DyNo ratings yet
- Jimenez vs. FranciscoDocument1 pageJimenez vs. FranciscoCzara DyNo ratings yet
- PNB Vs CA DigestDocument3 pagesPNB Vs CA DigestCzara DyNo ratings yet
- Syndrome Differentiation According To The Eight Principles - TCM Basic Principles ShennongDocument5 pagesSyndrome Differentiation According To The Eight Principles - TCM Basic Principles ShennongYi-Ying LuNo ratings yet
- NeuroblastomaDocument21 pagesNeuroblastomaRichard DjigoNo ratings yet
- Ketamine ZhaoPDocument12 pagesKetamine ZhaoPSutanMudaNo ratings yet
- (AIA) Hospital DESIGN GuidelinesDocument100 pages(AIA) Hospital DESIGN Guidelinespolyplop100% (1)
- Textbook of Pleural Diseases (2008)Document673 pagesTextbook of Pleural Diseases (2008)Alexandra NicaNo ratings yet
- HipersplenismDocument6 pagesHipersplenismDany YayanNo ratings yet
- Leukogram Patterns - EClinpathDocument6 pagesLeukogram Patterns - EClinpathCarlos YongNo ratings yet
- A Case For Psychiatric Leadership in Dispositional Capacity AssessmentDocument3 pagesA Case For Psychiatric Leadership in Dispositional Capacity AssessmentRicardo EscNo ratings yet
- 1cardiovascular and Pulmonary Physical TherapyDocument347 pages1cardiovascular and Pulmonary Physical TherapyLiviu CuvoiNo ratings yet
- Budson - Memory Loss, Alzheimer's Disease, and Dementia - 2 Ed - 2015Document283 pagesBudson - Memory Loss, Alzheimer's Disease, and Dementia - 2 Ed - 2015Nathaly Cantor100% (3)
- Dubai Healthcare Professional Licensing Guide - Final - 2Document141 pagesDubai Healthcare Professional Licensing Guide - Final - 2Fahad IqbalNo ratings yet
- From Hippo Crates To GalenDocument26 pagesFrom Hippo Crates To GalensalammiNo ratings yet
- PDEA S Register 2-14 FormDocument12 pagesPDEA S Register 2-14 FormAngelito BALUYOT JRNo ratings yet
- Desi Elage: High Cholestrol Level in Blood (Khoon Main Cholesterol Ka Level Barh Jae)Document7 pagesDesi Elage: High Cholestrol Level in Blood (Khoon Main Cholesterol Ka Level Barh Jae)Irshad HussainNo ratings yet
- Health Hazards of Chemicals Commonly Used On Military BasesDocument35 pagesHealth Hazards of Chemicals Commonly Used On Military Basesmale nurseNo ratings yet
- KLSC BDU Kuwait Healthcare Report 2019 VF PDFDocument16 pagesKLSC BDU Kuwait Healthcare Report 2019 VF PDFJim MacaoNo ratings yet
- Stewardship White PaperDocument21 pagesStewardship White PaperHosam GomaaNo ratings yet
- Irritable Bowel Syndrome CASE STUDY REVISEDDocument51 pagesIrritable Bowel Syndrome CASE STUDY REVISEDJenjen 23No ratings yet
- The Advanced Trauma Life Support Course: A History of Its Development and Review of Related LiteratureDocument5 pagesThe Advanced Trauma Life Support Course: A History of Its Development and Review of Related LiteratureAlphonse ThangapradeepNo ratings yet
- Gima CatalogDocument84 pagesGima Catalogsara şovreNo ratings yet
- Thrombosis Research: Letter To The Editors-in-ChiefDocument3 pagesThrombosis Research: Letter To The Editors-in-ChiefRia GandaNo ratings yet
- Dr. Ilham - AFLP - ISSHP 2017 BandungDocument40 pagesDr. Ilham - AFLP - ISSHP 2017 BandungMegaSariDewiNo ratings yet
- Kaqun Studies Book 2013 PDFDocument183 pagesKaqun Studies Book 2013 PDFVeres András100% (2)
- The Patient Was Taken To The Emergency RoomDocument2 pagesThe Patient Was Taken To The Emergency RoomAndika Ridho MNo ratings yet
- Pediatric Respiratory EmergenciesDocument36 pagesPediatric Respiratory EmergenciesAbu RidhuwanNo ratings yet
- Analgesic Policy (2009)Document84 pagesAnalgesic Policy (2009)Ramon MagsaysayNo ratings yet
- Patofisiologi, Gambaran Klinis, Dan Tata Laksana HIV - AIDS (Dr. Kurniyanto)Document60 pagesPatofisiologi, Gambaran Klinis, Dan Tata Laksana HIV - AIDS (Dr. Kurniyanto)OrflimeEmmyNo ratings yet
- Cattle Diseases Farmers GuideDocument77 pagesCattle Diseases Farmers GuideDivyajyoti DevaNo ratings yet
- Informatics and Nursing Sensitive Quality Indicators: Name Institution Date CourseDocument5 pagesInformatics and Nursing Sensitive Quality Indicators: Name Institution Date CourseKevin SangNo ratings yet
- Radiotherapy NursingDocument35 pagesRadiotherapy NursingMarlon Rey AnacletoNo ratings yet