You might also like
- Zambia PHF Exit Interview QuestionnaireDocument37 pagesZambia PHF Exit Interview QuestionnairenomdeplumNo ratings yet
- Ujian Ulang Me 2010Document16 pagesUjian Ulang Me 2010Adhy GunserNo ratings yet
- Sociological and Environmental Study of The Community Katukurunda 2Document2 pagesSociological and Environmental Study of The Community Katukurunda 2tharinduanjana323No ratings yet
- Format JiwaDocument16 pagesFormat JiwaiwanNo ratings yet
- Neurological Assessment ToolDocument11 pagesNeurological Assessment ToolRadha SriNo ratings yet
- Medical CertificateDocument4 pagesMedical CertificateRishi ScifreakNo ratings yet
- Client Consultation CardDocument3 pagesClient Consultation Cardapi-614534740100% (1)
- Thyroid CaseDocument3 pagesThyroid Caselune junieNo ratings yet
- Laporan Pemeriksaan Kesehatan Rs ParinduDocument5 pagesLaporan Pemeriksaan Kesehatan Rs ParinduPOKJA KKSNo ratings yet
- 2023-Aug-Thu - Medical Examination Form - AfyaDocument3 pages2023-Aug-Thu - Medical Examination Form - Afyamasoudmakame17No ratings yet
- Travel Questionnaire For PatientsDocument2 pagesTravel Questionnaire For PatientsVineet ShettyNo ratings yet
- All About Diabetes 20Document6 pagesAll About Diabetes 20chungoc0898No ratings yet
- COVID-19 Athlete Information FormDocument1 pageCOVID-19 Athlete Information FormGianluigi BuffonNo ratings yet
- Apendicita AcutaDocument2 pagesApendicita AcutaIoana GrayNo ratings yet
- MUHAS Medical Exam FormDocument2 pagesMUHAS Medical Exam FormLusungu S. LupenzaNo ratings yet
- Patients Chart UpdatedDocument3 pagesPatients Chart UpdatedVinco GonzalezNo ratings yet
- Health Fitness Certificate For The Purposes of Permission To Work in Confined SpaceDocument6 pagesHealth Fitness Certificate For The Purposes of Permission To Work in Confined SpaceNur ShaNo ratings yet
- Sport and HealthDocument1 pageSport and HealthOLevkeNo ratings yet
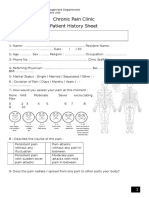
- Chronic Pain Clinic Patient History SheetDocument4 pagesChronic Pain Clinic Patient History SheetBelal N. MahfouzNo ratings yet
- FORM C Medical ExaminationDocument2 pagesFORM C Medical ExaminationBrilliant PaulNo ratings yet
- A Visit To The DoctorDocument8 pagesA Visit To The DoctorrifkaNo ratings yet
- Health Certificate WUCCDocument1 pageHealth Certificate WUCCsalsabila bara putriNo ratings yet
- Questionnaire 1Document13 pagesQuestionnaire 1Laeeq R MalikNo ratings yet
- Medical Assessment Form Blank-1Document4 pagesMedical Assessment Form Blank-1Zakiya HassanNo ratings yet
- Confidential: Medical History and Personal Particulars of Students Joining at IIT MadrasDocument4 pagesConfidential: Medical History and Personal Particulars of Students Joining at IIT MadrasNehaNo ratings yet
- Super Size Me 2Document2 pagesSuper Size Me 2Isabelle TheryNo ratings yet
- Assessment Form UnairDocument6 pagesAssessment Form UnairAkiel Shinobe SlopengNo ratings yet
- Access To and Utilisation of HIV Primary Care ServicesDocument2 pagesAccess To and Utilisation of HIV Primary Care ServicesCharro BayangNo ratings yet
- Targeted Patient Safety QuestionnairesDocument27 pagesTargeted Patient Safety QuestionnairesAafreen KhairNo ratings yet
- Community DiagnosisDocument10 pagesCommunity DiagnosisNestoryNo ratings yet
- Patient Hypertension SurveyDocument10 pagesPatient Hypertension SurveyIzaz KhanNo ratings yet
- Chest Stabbing DiagnosisDocument11 pagesChest Stabbing DiagnosisMustafa100% (1)
- 3.medical FormDocument5 pages3.medical Formamistudio30No ratings yet
- TN TRA Blood Donor QuestionnaireDocument2 pagesTN TRA Blood Donor QuestionnaireEman KarisNo ratings yet
- Admission Form For PatientsDocument4 pagesAdmission Form For PatientsShirley Dwi GayatriNo ratings yet
- Appendices: Appendix 1: Letter of Introduction and Questionnaires Expression of InterestDocument13 pagesAppendices: Appendix 1: Letter of Introduction and Questionnaires Expression of InterestmuhammaddaliiiNo ratings yet
- The Ultra Thyroid SolutionDocument58 pagesThe Ultra Thyroid Solutionnaginat100% (17)
- Proforma For MCCD CertificateDocument1 pageProforma For MCCD CertificateEXAM INFONo ratings yet
- UCEN LIC EN NUTRICIÓN INGLES 1 PARCIAL 1Document1 pageUCEN LIC EN NUTRICIÓN INGLES 1 PARCIAL 1Juan De Los SantosNo ratings yet
- Pelvic Pain Patient Initial QuestionnaireDocument6 pagesPelvic Pain Patient Initial QuestionnaireVaralakshmi UppuNo ratings yet
- Examen Unit 6Document4 pagesExamen Unit 6FranciscaBalasSuarezNo ratings yet
- Medical Fitness Certificate 9Document1 pageMedical Fitness Certificate 9Animal nutritionNo ratings yet
- Pre-Exercise Screening Form: 1.personal DetailsDocument4 pagesPre-Exercise Screening Form: 1.personal DetailsLee TarrozaNo ratings yet
- Family doctor registration formDocument6 pagesFamily doctor registration formJervan KhouNo ratings yet
- Fitness FormDocument2 pagesFitness FormkaramatNo ratings yet
- CD-42 - Medical QuestionnaireDocument6 pagesCD-42 - Medical QuestionnaireRasLDKNo ratings yet
- 14.05 Eurojam-Health Sheet GB FRDocument3 pages14.05 Eurojam-Health Sheet GB FRZanfir MihailNo ratings yet
- Blood Donation Application FormDocument2 pagesBlood Donation Application FormFadjar MulyaNo ratings yet
- Case Postpartum PeriodDocument8 pagesCase Postpartum PeriodAhmed SabryNo ratings yet
- Bahasa Inggris SOALDocument20 pagesBahasa Inggris SOALAyu Nita PangestuNo ratings yet
- LIVING WILL (Sample 1) : Willfully andDocument3 pagesLIVING WILL (Sample 1) : Willfully andChristopher FungNo ratings yet
- Unit 10 ReviewDocument3 pagesUnit 10 Review16. Nguyễn Thùy LinhNo ratings yet
- Medical Clearance FormDocument2 pagesMedical Clearance FormPhake CodedNo ratings yet
- Test 1 Model 1 English 2 Bac First Term 8Document4 pagesTest 1 Model 1 English 2 Bac First Term 8Fatyma ZahraeNo ratings yet
- A Rational Approach 2 ND EditionDocument125 pagesA Rational Approach 2 ND Editionstephanie_bonner_2100% (2)
- Perinatal-Neonatal Death Reporting FormDocument4 pagesPerinatal-Neonatal Death Reporting FormLusye AmaliaNo ratings yet
- Sana'a University Faculty of Medicine Smart Sheets for History TakingDocument76 pagesSana'a University Faculty of Medicine Smart Sheets for History Takingruba al hammadiNo ratings yet
- Dengue Pre Vaccination Screening and Positive PredDocument3 pagesDengue Pre Vaccination Screening and Positive PredSimbakutty VenkataramananNo ratings yet
- Multidrug Resistant Tuberculosis Outbreak in South 7Document2 pagesMultidrug Resistant Tuberculosis Outbreak in South 7Simbakutty VenkataramananNo ratings yet
- Low Anti Rubella Antibody Levels in Public FacilitDocument1 pageLow Anti Rubella Antibody Levels in Public FacilitSimbakutty VenkataramananNo ratings yet
- 30.07.2021 RDC C Daily ReportDocument78 pages30.07.2021 RDC C Daily ReportSimbakutty VenkataramananNo ratings yet
- 4 5949683011053161120Document5 pages4 5949683011053161120Simbakutty VenkataramananNo ratings yet
- 30.07.2021 - RDC C Daily ReportDocument71 pages30.07.2021 - RDC C Daily ReportSimbakutty VenkataramananNo ratings yet
- Above 80 Age Not 2 Dose Not Vaccinated DetailsDocument4 pagesAbove 80 Age Not 2 Dose Not Vaccinated DetailsSimbakutty VenkataramananNo ratings yet
- Above 80 Age Not Vaccinated DetailsDocument9 pagesAbove 80 Age Not Vaccinated DetailsSimbakutty VenkataramananNo ratings yet
- 30.07.2021 - RDC C Daily ReportDocument69 pages30.07.2021 - RDC C Daily ReportSimbakutty VenkataramananNo ratings yet
- 30.07.2021 - RDC C Daily ReportDocument69 pages30.07.2021 - RDC C Daily ReportSimbakutty VenkataramananNo ratings yet
- 30.07.2021 - RDC C Daily ReportDocument71 pages30.07.2021 - RDC C Daily ReportSimbakutty VenkataramananNo ratings yet
- Telemedicine Equipment SpecificationsDocument20 pagesTelemedicine Equipment SpecificationsSimbakutty VenkataramananNo ratings yet
- ChickenpoxDocument6 pagesChickenpoxlolytaindahNo ratings yet
- Steps To Cast Your Vote For GPGAOWA Election 2020-2022 PDFDocument3 pagesSteps To Cast Your Vote For GPGAOWA Election 2020-2022 PDFSimbakutty VenkataramananNo ratings yet
- 27.07.2021 - RDC C Daily ReportDocument88 pages27.07.2021 - RDC C Daily ReportSimbakutty VenkataramananNo ratings yet
- 1 BellsPalsy PDFDocument14 pages1 BellsPalsy PDFSimbakutty VenkataramananNo ratings yet
- Covid Positive Case Details from Various AddressesDocument27 pagesCovid Positive Case Details from Various AddressesSimbakutty VenkataramananNo ratings yet
- Model QP - Grade VII - Jiji PDFDocument4 pagesModel QP - Grade VII - Jiji PDFSimbakutty VenkataramananNo ratings yet
- Neet Committee PDFDocument16 pagesNeet Committee PDFSimbakutty VenkataramananNo ratings yet
- 9th-Phy-Shift 2Document17 pages9th-Phy-Shift 2TanyaNo ratings yet
- CBSE Class 11 Chemistry Sample Paper Set A PDFDocument6 pagesCBSE Class 11 Chemistry Sample Paper Set A PDFSimbakutty VenkataramananNo ratings yet
- The Tamil Nadu Government Servants' Conduct Rules, 1973update Mar 10Document42 pagesThe Tamil Nadu Government Servants' Conduct Rules, 1973update Mar 10RAJAGURU.VNo ratings yet
- TB DCP-B7500D PDFDocument2 pagesTB DCP-B7500D PDFSimbakutty VenkataramananNo ratings yet
- 4 OverviewBrightonMethods Vaccine 2007Document4 pages4 OverviewBrightonMethods Vaccine 2007Simbakutty VenkataramananNo ratings yet
- Class 7 Maths Integers: Natural NumbersDocument11 pagesClass 7 Maths Integers: Natural NumbersSimbakutty VenkataramananNo ratings yet
- 2 Bonhoeffer 2002 Vaccine PDFDocument6 pages2 Bonhoeffer 2002 Vaccine PDFSimbakutty VenkataramananNo ratings yet
- Handicap Rail FormDocument1 pageHandicap Rail FormjdpaniNo ratings yet
- Brighton's Classification For AEFI CasesDocument2 pagesBrighton's Classification For AEFI CasesSimbakutty VenkataramananNo ratings yet
- Standardized Case Definitions of Adverse Events Following Immunization (AEFI)Document4 pagesStandardized Case Definitions of Adverse Events Following Immunization (AEFI)Simbakutty VenkataramananNo ratings yet
- Brighton’s Classification for AEFI casesDocument7 pagesBrighton’s Classification for AEFI casesSimbakutty VenkataramananNo ratings yet
- KTS - Sarao.bakus Temple of Eternal FiireDocument176 pagesKTS - Sarao.bakus Temple of Eternal FiireK.T.S. SaraoNo ratings yet
- Great Gatsby Study NotesDocument69 pagesGreat Gatsby Study NotesLara Westwood100% (2)
- Fe in Black TeaDocument6 pagesFe in Black TeaHerni Nur AeniNo ratings yet
- Type 2 Diabetes MellitusDocument6 pagesType 2 Diabetes MellitusJoy NisoladaNo ratings yet
- Paradise Pools Flyer With Price ListDocument5 pagesParadise Pools Flyer With Price ListKhuzaima HussainNo ratings yet
- Mathematics: Minimum Level Learning MaterialDocument60 pagesMathematics: Minimum Level Learning MaterialTusar SardarNo ratings yet
- Journal of Alloys and Compounds: Wei Li, Zhijun Xu, Ruiqing Chu, Peng Fu, Guozhong ZangDocument4 pagesJournal of Alloys and Compounds: Wei Li, Zhijun Xu, Ruiqing Chu, Peng Fu, Guozhong ZangSamah SamahNo ratings yet
- Modicon TM172PDG42R DatasheetDocument14 pagesModicon TM172PDG42R DatasheetRonnie SolomonNo ratings yet
- Kirloskar-Oil-Engines DescriptionsDocument8 pagesKirloskar-Oil-Engines Descriptionssinghhardeep760No ratings yet
- (Computing 14) A. Aguilera, D. Ayala (Auth.), Professor Dr. Guido Brunnett, Dr. Hanspeter Bieri, Professor Dr. Gerald Farin (Eds.) - Geometric Modelling-Springer-Verlag Wien (2001)Document356 pages(Computing 14) A. Aguilera, D. Ayala (Auth.), Professor Dr. Guido Brunnett, Dr. Hanspeter Bieri, Professor Dr. Gerald Farin (Eds.) - Geometric Modelling-Springer-Verlag Wien (2001)ANDRES Fernando Mosquera DIAZNo ratings yet
- Metric Heavy Hex Nuts: ASME B18.2.4.6M-2010Document16 pagesMetric Heavy Hex Nuts: ASME B18.2.4.6M-2010CarlitosNo ratings yet
- MATERIAL SAFETY DATA SHEET FOR PREVENTOL-D6 PRESERVATIVEDocument3 pagesMATERIAL SAFETY DATA SHEET FOR PREVENTOL-D6 PRESERVATIVEAkshay PushpanNo ratings yet
- Eng ThreePDocument192 pagesEng ThreePMr Ahmed AbdallahNo ratings yet
- Nokia N97 User Guide: 9221217 Issue 2.0Document76 pagesNokia N97 User Guide: 9221217 Issue 2.0Boris CavarNo ratings yet
- Engineering Mechanics Lectures PDFDocument83 pagesEngineering Mechanics Lectures PDFluay adnanNo ratings yet
- Large and Medium Manufacturing Industry Survey Report 2018Document778 pagesLarge and Medium Manufacturing Industry Survey Report 2018melakuNo ratings yet
- Earthbag House For HaitiDocument22 pagesEarthbag House For HaitiRaymond KatabaziNo ratings yet
- Warhammer 40k Kroot VehiclesDocument2 pagesWarhammer 40k Kroot VehiclesJoseph RobinsonNo ratings yet
- JMJ Marist Brothers Notre Dame of Marbel University Integrated Basic Education Department City of Koronadal, South CotabatoDocument13 pagesJMJ Marist Brothers Notre Dame of Marbel University Integrated Basic Education Department City of Koronadal, South CotabatoNestor Gerotape DiosanaNo ratings yet
- PRN Maths Midterm QP Aug 18Document3 pagesPRN Maths Midterm QP Aug 18JanakChandPNo ratings yet
- Hobby 01: COD. 9942062.01 REV. 00Document9 pagesHobby 01: COD. 9942062.01 REV. 00Alexander SharamiginNo ratings yet
- Analytical Mechanics SolutionsDocument193 pagesAnalytical Mechanics SolutionsQuinton Boltin67% (9)
- Vapour Bar Exchange IMFL PackageDocument4 pagesVapour Bar Exchange IMFL PackageNishank AgarwalNo ratings yet
- Manual of Curatorship: A Guide To Museum PracticeDocument7 pagesManual of Curatorship: A Guide To Museum PracticeLuísa MenezesNo ratings yet
- อัตราภาษีของไทยที่ลดให้เปรูDocument124 pagesอัตราภาษีของไทยที่ลดให้เปรูDante FilhoNo ratings yet
- SAFETY AND LOSS PREVENTION FOR CHEMICAL PROCESS FACILITIESDocument13 pagesSAFETY AND LOSS PREVENTION FOR CHEMICAL PROCESS FACILITIESKinosraj KumaranNo ratings yet
- Chapter 3 (CHM 127)Document105 pagesChapter 3 (CHM 127)FiqajasmeNo ratings yet
- FHM Espana 2010 12 PDFDocument2 pagesFHM Espana 2010 12 PDFBrandenNo ratings yet
- F588 PDFDocument8 pagesF588 PDFOscar Gutiérrez-JuncoNo ratings yet
- Deam Edan M8 Monitor - User ManualDocument248 pagesDeam Edan M8 Monitor - User Manualvelasquez diazNo ratings yet