You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Art:10.1007/s12663 012 0335 0Document5 pagesArt:10.1007/s12663 012 0335 0AshishRajputNo ratings yet
- Joms2004 Tetracyline PDFDocument5 pagesJoms2004 Tetracyline PDFAshishRajputNo ratings yet
- Third Molar Position: Reliability of Panoramic RadiographyDocument6 pagesThird Molar Position: Reliability of Panoramic RadiographyAshishRajputNo ratings yet
- Resume: Name-Mr. Kailash Anandsingh Pardeshi. Education - M.A. English (Entire) M.A. Pali, L.L.B, PGDM in ExperienceDocument1 pageResume: Name-Mr. Kailash Anandsingh Pardeshi. Education - M.A. English (Entire) M.A. Pali, L.L.B, PGDM in ExperienceAshishRajputNo ratings yet
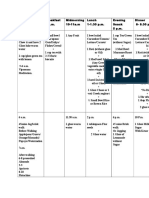
- Papa Diet PlanDocument2 pagesPapa Diet PlanAshishRajputNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Group H (Sn.8) Lab ReportDocument152 pagesGroup H (Sn.8) Lab ReportNishrita DevnathNo ratings yet
- danarobu,+EE+40+2+2021 29Document11 pagesdanarobu,+EE+40+2+2021 29Buzoianu Ovidiu Andrei CristianNo ratings yet
- Thesis Presentation Slides UNIBGDocument33 pagesThesis Presentation Slides UNIBGRomeo DanielsNo ratings yet
- Checklist Audit Factorial HRDocument2 pagesChecklist Audit Factorial HRSoraya AisyahNo ratings yet
- 2nd Quarter Review 4Document135 pages2nd Quarter Review 4Prenrose Deferia PiaNo ratings yet
- Case Study Data Analytics by RevoU 1659413996Document11 pagesCase Study Data Analytics by RevoU 1659413996Vicky NopatNo ratings yet
- Activities For LEGO WeDo With Scratch ScriptsDocument5 pagesActivities For LEGO WeDo With Scratch ScriptsFelipe SousaNo ratings yet
- Digital Door Lock System MarketDocument11 pagesDigital Door Lock System MarketNamrataNo ratings yet
- Lecture03 Informed SearchDocument41 pagesLecture03 Informed SearchRohan ZahidNo ratings yet
- PSA QB 15-16 With AnswerDocument75 pagesPSA QB 15-16 With Answerkmohanadasse100% (1)
- Modeling Transition State in GaussianDocument5 pagesModeling Transition State in GaussianBruno Moraes ServilhaNo ratings yet
- Advantages and Disadvantages of Object-Oriented Programming (OOP)Document2 pagesAdvantages and Disadvantages of Object-Oriented Programming (OOP)anruagNo ratings yet
- TDA7442 TDA7442D: Tone Control and Surround Digitally Controlled Audio ProcessorDocument17 pagesTDA7442 TDA7442D: Tone Control and Surround Digitally Controlled Audio ProcessorTorikul HabibNo ratings yet
- 2SC2022 KTC2022 BrotherDocument2 pages2SC2022 KTC2022 Brotherxerox4512No ratings yet
- Fundamentals of PLCs ReviewDocument65 pagesFundamentals of PLCs ReviewPatrickSchardt100% (2)
- DatasheetDocument36 pagesDatasheetErick EmersonNo ratings yet
- RACH ProcessDocument11 pagesRACH ProcessSwayam SambitNo ratings yet
- 02 Awareness of Information Security For New Employee)Document30 pages02 Awareness of Information Security For New Employee)Yens ContrerasNo ratings yet
- Salesforce Data Architect Certification GuideDocument254 pagesSalesforce Data Architect Certification Guideglm.mendesrNo ratings yet
- Flow Formerly Open Source CRV v1Document72 pagesFlow Formerly Open Source CRV v1Dragon LordNo ratings yet
- Dlp-For-Life Shashi Mae BonifacioDocument20 pagesDlp-For-Life Shashi Mae BonifacioShashi Mae BonifacioNo ratings yet
- Switchgears & Fuse: HSN Codes and Corresponding GST% For Electrical Items Supplied by Us - July 21, 2017Document2 pagesSwitchgears & Fuse: HSN Codes and Corresponding GST% For Electrical Items Supplied by Us - July 21, 2017sasasjkNo ratings yet
- Customer Relationship ManagementDocument4 pagesCustomer Relationship ManagementArishima RareryNo ratings yet
- Assignment 2 Sem 1Document6 pagesAssignment 2 Sem 1d_systemsugandaNo ratings yet
- Russian Codes: Catalog of Regulations Available To OrderDocument1 pageRussian Codes: Catalog of Regulations Available To Ordervemps36No ratings yet
- CompTIA Security Certification Practice Test 2 Exam SY0 601Document5 pagesCompTIA Security Certification Practice Test 2 Exam SY0 601Allondra Lado-anNo ratings yet
- AeroCut Prime OPERATION MANUAL (XX-XXX) (E)Document52 pagesAeroCut Prime OPERATION MANUAL (XX-XXX) (E)Dascalu AndreiNo ratings yet
- Manual NTWDocument24 pagesManual NTWElias Melo JrNo ratings yet
- SARJournalMarch2022 52 62Document11 pagesSARJournalMarch2022 52 62Harambe GorillaNo ratings yet
- ADE7566Document136 pagesADE7566An Huynh VanNo ratings yet